
Key Takeaways
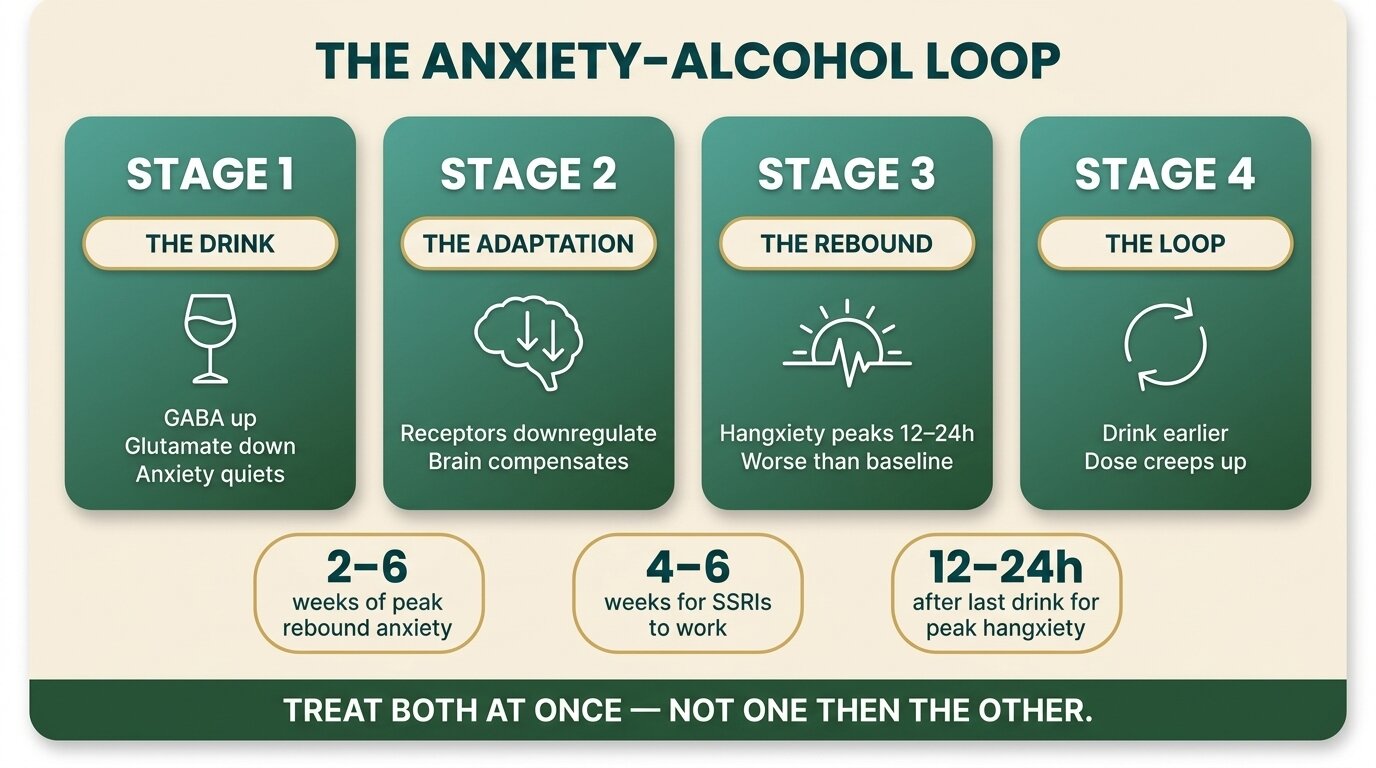
- Many people drink to quiet anxiety — alcohol lifts GABA and lowers glutamate in the moment, but the brain adapts within weeks, leaving you with rebound anxiety the next morning that is often worse than where you started.
- “Just stopping” rarely works because the original anxiety disorder usually predates the drinking. Cut the alcohol out cold and the underlying panic comes back, full strength, around weeks 2–6 of sobriety.
- Integrated treatment — treating the anxiety and the alcohol use at the same time — produces better outcomes than treating either alone (Smith & Randall, Alcohol Research, 2012).
- SSRIs and SNRIs are the usual first-line medications for the anxiety side. Daily benzodiazepines are avoided — they share alcohol’s mechanism and create a worse dependence than the one you started with.
- One Step Rehab in Chiang Mai runs an integrated CBT and medication-management programme with a consultant psychiatrist, group therapy, and on-site detox for the alcohol withdrawal that triggers most relapse.
If you drink to take the edge off your anxiety, you are not unusual and you are not weak — you are stuck in a loop with a name. Alcohol calms anxiety in the short term by amplifying GABA, the brain’s main inhibitory signal, but the brain compensates within weeks. GABA receptors downregulate, glutamate activity climbs, and the next morning the anxiety rebounds harder than baseline (Brady & Sinha, Am J Psychiatry, 2005). Each drink fixes less and costs more. Eventually the drinking becomes its own problem, stacked on top of the anxiety you were trying to manage in the first place.
This is one of the most common patterns we see at One Step. It rarely responds to willpower, and it rarely responds to standalone anxiety treatment — meditation apps, yoga, CBT in isolation. It responds to integrated dual diagnosis treatment: addressing the anxiety and the alcohol use in parallel, with the right medications and the right therapy, in an environment where the dangerous early-sobriety window is protected.
How Does Alcohol Become a Way to Self-Medicate Anxiety?
Alcohol works on anxiety the same way a sedative does: it depresses the central nervous system, amplifies GABA, and suppresses glutamate. The effect is real and immediate, which is why it works once. The problem is that the brain adapts within weeks — GABA receptors become less sensitive, glutamate activity climbs, and you wake up with rebound anxiety worse than baseline. The fix becomes the cause.
This is what researchers call the self-medication hypothesis, and for anxiety disorders it has strong evidence behind it. Kushner and colleagues described the mechanism plainly: short-term anxiety reduction from alcohol, combined with long-term anxiety induction from chronic drinking and withdrawal, creates a vicious feed-forward cycle (Kushner et al., Clin Psychol Rev, 2000). The dose creeps up. “One glass of wine at 7pm” becomes two glasses at 6pm becomes a bottle starting at 5pm. Tolerance climbs faster than people expect, and the rebound on non-drinking days starts to feel intolerable.
For the high-functioning anxious drinker — often a professional, often someone who has already tried meditation, yoga, and self-help books — this loop is usually invisible until it isn’t. Work performance holds up. Social life looks normal. But the drinking has become structural: not a treat, not a habit, but the only reliable way to come down from the day. By the time it shows up as a problem, the anxiety and the alcohol use are tangled together, and untangling them needs both ends pulled at once.
Why Doesn’t Quitting Drinking Fix the Underlying Anxiety?
Because the anxiety usually came first. Most people who self-medicate with alcohol have an untreated anxiety disorder that predates the drinking — generalised anxiety, panic disorder, social anxiety, or PTSD. Stopping the alcohol removes the suppressant, and the anxiety it was masking comes back at full volume. This is the dangerous part of early sobriety, and it is where most relapse happens.
What people experience in weeks 2–6 of abstinence often surprises them. The acute alcohol withdrawal has passed, the shakes and the racing heart are gone, but the panic gets worse, not better. Sleep is broken. Mornings feel intolerable. The conviction that “drinking is the only thing that ever helped” rises sharply, which is why this window is the most common relapse point (Brady & Sinha, Am J Psychiatry, 2005).
This is also where the standard “treat the alcohol first, see if the anxiety resolves” approach fails. NICE CG115 recommends three to four weeks of abstinence before reassessing anxiety symptoms — sensible in theory, but only workable if the person makes it through those weeks without drinking again. For someone with a real anxiety disorder underneath, three to four weeks unmedicated and unsupported is a long time. Many do not make it. The integrated approach is to start treating the anxiety in parallel — with appropriate medication and therapy — from the start of abstinence, not after it.

What Actually Happens in Your Brain Between the Last Drink and the Next Morning?
Alcohol amplifies GABA and suppresses glutamate. The brain compensates by reducing GABA sensitivity and increasing glutamate activity. When the alcohol wears off, GABA is still suppressed and glutamate is running high — the brain is hyperexcitable. That is what rebound anxiety is, and it usually peaks 12 to 24 hours after the last drink.
Three things are useful to understand about this:
| Phase | What’s happening in the brain | What you feel |
|---|---|---|
| First drinks of the night | GABA amplified, glutamate suppressed | Calm, social, less anxious |
| As alcohol leaves the system (4–12 hrs) | Brain over-compensates; glutamate climbs | Light sleep, anxious dreams, early waking |
| Morning after (12–24 hrs) | GABA still suppressed, glutamate elevated | “Hangxiety” — racing heart, dread, panic |
| Chronic daily drinking (weeks/months) | Permanent receptor adaptation | Baseline anxiety higher than before drinking started |
| Early sobriety (weeks 2–6) | Receptors slowly resetting | Worst anxiety yet — peak relapse window |
This is why people who try to taper or “just cut back” often feel worse than people who stop completely with support. Half-measures keep the receptor system constantly stressed without ever letting it reset. And it is why the early sobriety window is the most important one to protect — not because the physical detox is dangerous (for moderate drinkers, it usually isn’t) but because the anxiety is at its peak and the relapse risk is at its peak at the same time.
Which Medications Actually Help Anxiety in Early Sobriety?
The first-line options for treating anxiety in someone who has just stopped drinking are SSRIs (sertraline, escitalopram) and SNRIs (venlafaxine, duloxetine). These take four to six weeks to reach full effect, which means starting them early — during the late stage of detox or the first week of abstinence — so they are working by the time the peak rebound anxiety arrives at weeks 2–6.
What the medication options look like in practice:
| Medication | Where it fits | Notes |
|---|---|---|
| SSRIs (sertraline, escitalopram) | First-line for generalised anxiety, panic, social anxiety | Slow onset (4–6 weeks). Start during detox if possible. |
| SNRIs (venlafaxine, duloxetine) | Alternative when SSRIs don’t suit | Useful when low mood is also prominent. |
| Buspirone | Add-on for chronic anxiety, no abuse potential | Modest effect, slow onset, but very safe. |
| Hydroxyzine | Situational, non-addictive sedative-antihistamine | Good for sleep and acute episodes without dependence risk. |
| Propranolol | Physical symptoms — racing heart, tremor | Useful for situational anxiety (presentations, flights). |
| Naltrexone | For the alcohol craving side | Reduces reward from drinking; can be combined with an SSRI. |
| Daily benzodiazepines (Xanax, Klonopin, Valium) | Avoided where possible | Same GABA mechanism as alcohol — cross-tolerance, dependence, worse rebound. |
The Cochrane review on antidepressants for co-occurring depression and alcohol dependence found low-quality evidence of benefit, with SSRIs showing modest effects on drinking outcomes when combined with psychological treatment (Agabio et al., Cochrane Database, 2018). The pattern in the anxiety literature is similar: medication helps, but it helps most when paired with CBT or another structured therapy, not on its own.
One thing matters more than any of the medication choices: do not switch from drinking every night to taking a benzodiazepine every day. Daily Xanax, Klonopin, or Valium uses the same GABA receptor that alcohol uses, creates the same cross-tolerance, and produces a withdrawal that is medically more dangerous than alcohol withdrawal. It is the worst trap to fall into during early sobriety, and it happens more than it should because benzos work fast and SSRIs are slow.
The single biggest mistake I see is people swapping alcohol for daily benzodiazepines because the anxiety in early sobriety feels unbearable. It almost always ends in a worse dependence than the one we started treating. The harder, slower answer is to bring an SSRI or SNRI on board early, accept that the first six weeks will be uncomfortable, and use therapy, structure, and non-addictive medications like buspirone or hydroxyzine to get through the window.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Which Therapies Work for Anxiety and Alcohol Use at the Same Time?
Cognitive behavioural therapy (CBT) is the strongest-evidence approach for both anxiety and alcohol use disorder, and the same therapist can treat both in integrated sessions. Exposure-based work is added when avoidance is driving the drinking. Mindfulness-based relapse prevention helps with the urge-surfing skill. EMDR is added when trauma sits underneath the anxiety.
Smith and Randall’s review of the literature makes the same point clinicians see in practice: integrated treatment — addressing both disorders in parallel rather than sequentially — produces better outcomes than treating either condition alone (Smith & Randall, Alcohol Research, 2012). SAMHSA’s clinical guidance for co-occurring disorders takes the same position: substance use disorders and mental disorders should be treated concurrently, not in a queue (SAMHSA TIP 42, 2020).
What “integrated” actually looks like in a residential setting:
- Daily CBT sessions that target both the anxiety triggers and the drinking triggers in the same session — because they are usually the same triggers.
- Exposure work for the social situations, work situations, or internal sensations the person was drinking to avoid.
- Mindfulness and urge-surfing skills for the moments when the body wants alcohol and there isn’t a therapist in the room.
- EMDR or trauma-focused therapy when the anxiety has roots in specific past events — common in this group.
- Group therapy for the loneliness piece. Many high-functioning anxious drinkers have built a life that looks full but doesn’t include anyone they can be honest with. Group breaks that.
For more on how CBT and DBT differ and which fits which presentation, see our breakdown of CBT vs DBT for addiction.
Not sure if integrated dual-diagnosis treatment is the right fit? Talk to our team — we’ll give you a straight answer about whether anxiety and alcohol together is something we treat well, or whether you’d be better served elsewhere.
Why Does Residential Treatment Help This Specific Pattern?
Because the most dangerous part of recovery — the rebound anxiety window at weeks 2–6 — happens at exactly the point where outpatient care drops off. In residential treatment that window is structured: daily therapy, set wake and sleep times, no easy access to alcohol, no isolation. The structure does the work that willpower cannot.
What the residential setting protects you from is not the urge to drink in a vacuum. It is the specific combination of peak anxiety + low support + cued environment that pushes people back to the bottle. At home, weeks 2–6 of sobriety look like: anxiety climbing, sleep poor, work demanding, the wine shop on the way home from the office. In residential treatment, weeks 2–6 look like: anxiety still climbing, but daily therapy on it, no wine shop, and seven other people in the room who are in the same week as you.
A 2018 review of the evidence on residential versus outpatient treatment for dual diagnosis found that residential settings produce better short-term outcomes for clients with significant anxiety symptoms because the daily therapeutic dose is higher and the environmental triggers are removed. We’ve written separately about why residential treatment works better than outpatient for this profile.

What Does One Step Rehab Do for Anxiety and Alcohol Together?
One Step runs an integrated dual diagnosis programme — daily CBT and group therapy, medication management with a consultant psychiatrist, and on-site detox for moderate alcohol withdrawal. The programme is residential, 28 to 60 days for most clients, structured from 7am to 9pm. The fee is approximately ฿280,000/month (~$8,500 USD), with medication, flights, and personal items billed separately.
The clinical setup for the anxious-drinker profile specifically:
- Intake psychiatric assessment with our consultant psychiatrist within the first 48 hours. The medication conversation happens early — usually starting an SSRI or SNRI during detox so it has time to work by the time peak rebound anxiety arrives.
- On-site detox for moderate alcohol dependence. For severe alcohol withdrawal — heavy daily drinking, history of seizures or DTs — we may detox you first at our partner hospital, which has intensive and intermediary intensive care units, before you transfer to One Step for the rehab programme.
- Daily individual CBT with a therapist who treats the anxiety and the drinking in the same session, because for this client group they are the same problem.
- Group therapy — the loneliness piece. Most high-functioning drinkers haven’t told anyone how much they drink. Group is where that comes out and where the isolation breaks.
- Structured daily schedule — see our treatment schedule. Wake times, meals, therapy, exercise, sleep. Routine is therapy for anxiety, especially in the first weeks.
- Aftercare planning from week three onward, including the medication handover to a community psychiatrist back home. See our aftercare programme.
For a fuller picture of how dual diagnosis is structured at One Step, see our overview of personalised dual diagnosis options and the types of dual diagnosis therapies we use. For the alcohol side specifically, our alcohol treatment programme and our breakdowns of what to expect from alcohol detox and the side effects of detoxification cover the medical side.
What the programme fee does not include: medications prescribed during your stay (you pay separately for what the psychiatrist prescribes — refills, new prescriptions, or supplements), flights, visa fees, hospital visits if severe detox is needed, additional counselling beyond the programme, and personal items. The pricing page (/pricing/) is the source of truth on what is and isn’t covered.

What’s a Realistic Timeline for Anxiety to Improve in Recovery?
For most clients with the anxiety-and-alcohol pattern, anxiety gets worse before it gets better. The first one to two weeks are dominated by acute withdrawal. Weeks 2 to 6 are the peak rebound window — the hardest. By month three, most people are noticeably more stable, and full benefit of treatment and medication usually arrives between months six and twelve.
| Phase | What’s happening | What helps |
|---|---|---|
| Week 1 | Acute withdrawal — shakes, sweats, racing heart, broken sleep | Medical detox, hydration, short-course tapered medication if needed |
| Weeks 2–6 | Rebound anxiety peaks. Often worse than baseline drinking | Daily therapy, structured day, SSRI starting to work, group support |
| Months 2–3 | Anxiety levelling off, sleep improving | Continued therapy, exercise, aftercare planning |
| Months 4–6 | Baseline below pre-drinking levels for most | Step-down therapy, community support, medication review |
| Months 6–12 | Full benefit of treatment realised | Long-term aftercare, relapse prevention plan, periodic medication review |
If nobody told you this timeline before, that’s the most common failure of standalone outpatient treatment for this pattern. People expect to feel better in week two, feel worse instead, and conclude that sobriety doesn’t work. It does — but the curve runs through some uncomfortable territory first, and it is much easier to walk that curve inside a programme than outside one. For practical strategies during this window, see our guide to the most common relapse triggers and how to plan for each and our piece on rebuilding sleep without alcohol.
Frequently Asked Questions
Common questions about anxiety, alcohol, and dual diagnosis treatment.
Not at first. Drinking to take the edge off is common and not automatically a disorder. It crosses into alcohol use disorder when the dose climbs, you can’t reliably stop or cut back, drinking starts to interfere with work or relationships, or you feel worse on non-drinking days than drinking days. By that point, the anxiety and the drinking are tangled and need integrated treatment.
For some people, yes — if the anxiety was entirely alcohol-induced, three to four weeks of abstinence may clear it. For most people who fit the “wine o’clock” self-medication pattern, no — the anxiety was there first and stopping reveals it. That is why an integrated approach treats both at once rather than waiting to see if the anxiety resolves on its own.
Daily benzodiazepine use is avoided in this situation. Benzos work on the same GABA receptor as alcohol, create the same cross-tolerance, and produce a withdrawal that is medically more dangerous than alcohol withdrawal. Short-term use during medical detox is sometimes appropriate; long-term daily use is usually swapping one dependence for a worse one.
This is rebound anxiety from GABA receptor downregulation and elevated glutamate activity, combined with the original anxiety disorder no longer being masked by alcohol. It typically peaks between weeks two and six and is the most common relapse point. It is also temporary, and it is one of the strongest reasons to be in structured treatment during that window.
SSRIs typically take four to six weeks to reach full anxiety benefit, and side effects often peak in the first two weeks before easing. In recovery, this is why they are usually started during detox or the first week of abstinence — so they are working by the time peak rebound anxiety arrives. Hydroxyzine or propranolol can bridge the gap for situational anxiety while the SSRI builds up.
Yes, for moderate alcohol dependence we run detox on-site with medical supervision during the acute phase. For severe alcohol dependence — heavy daily drinking, prior seizures, prior delirium tremens — we may detox you first at our partner hospital, which has intensive and intermediary intensive care units, before you transfer to One Step for the rehab programme.
Not necessarily. Morning-after anxiety (sometimes called “hangxiety”) is a withdrawal phenomenon driven by GABA-glutamate rebound and resolves as alcohol clears. A panic disorder produces sudden panic attacks independent of drinking. Many people have both — a true panic disorder that they were drinking to manage, and a hangxiety pattern on top of it. A psychiatric assessment is the only reliable way to separate them.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








