
Key Takeaways
- Around half of women in substance use treatment have a current or past eating disorder — the overlap is the rule, not the exception (SAMHSA, 2026).
- Treating addiction first and “dealing with the eating disorder later” often backfires. The eating disorder uses the same regulatory function the substance was providing, and intensifies in early sobriety.
- Integrated treatment works when the person is medically stable: moderate bulimia, binge eating disorder, or partly weight-restored anorexia alongside alcohol or stimulant misuse.
- It does not work when the eating disorder is medically dangerous: very low BMI, severe purging with electrolyte derangement, or anyone needing nasogastric tube feeding or refeeding syndrome monitoring. Those cases need a specialised eating disorder unit first.
- At One Step we run integrated CBT for eating disorders (CBT-E) alongside addiction-focused CBT, supervised meals, and shared case formulation with our consultant psychiatrist. We do not run a locked eating disorder unit and we are not the right setting for acute medical instability.
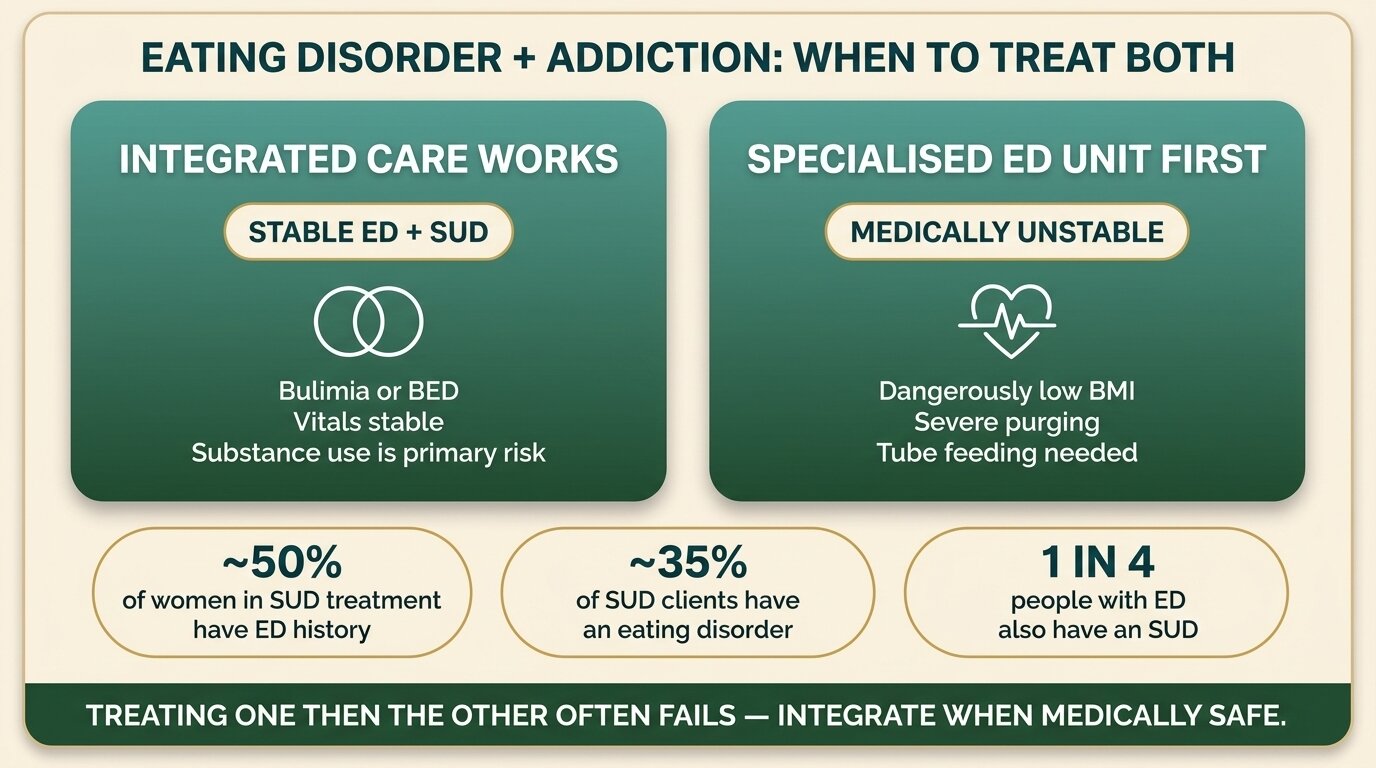
If you have both an eating disorder and a substance use problem, you need treatment that addresses both at the same time — not one and then the other. The two conditions reinforce each other through shared reward circuitry, shared distress, and shared coping function. Treating one in isolation usually causes the other to get worse. About 50% of women in substance use treatment also have a history of disordered eating, and about 35% of people with substance use disorders have a co-occurring eating disorder (SAMHSA, 2026).
This post explains when integrated residential treatment is the right call, when a specialised eating disorder unit needs to come first, and exactly what One Step Rehab does and does not provide for clients with both diagnoses.
How Often Do Eating Disorders and Substance Use Co-Occur?
Eating disorders and substance use disorders overlap far more than most rehabs acknowledge. SAMHSA’s 2026 advisory reports that more than 1 in 4 people with an eating disorder also meet criteria for a substance use disorder, up to 35% of people with substance use disorders have a co-occurring eating disorder, and the rate climbs to roughly 50% among women in addiction treatment (SAMHSA, 2026).
The pattern is consistent across the research. A systematic review and meta-analysis of nearly fifty studies found a pooled lifetime rate of substance use disorder among people with eating disorders of 21.9%, with alcohol the most common drug at 20.6% prevalence and the highest rates in people with binge-purge presentations (Bahji et al., Psychiatry Research, 2019). A separate review of women specifically reported substance use rates among those with eating disorders ranging from 8% to 42% depending on the eating disorder subtype, with bulimia and binge-purge anorexia carrying the highest risk (Harrop and Marlatt, Addictive Behaviors, 2010).
| Eating disorder | Most common co-occurring substance | Lifetime SUD rate (approx) |
|---|---|---|
| Bulimia nervosa | Alcohol, stimulants | 30–50% |
| Binge eating disorder | Alcohol, cannabis | 20–25% |
| Anorexia (binge-purge subtype) | Stimulants, alcohol | 25–40% |
| Anorexia (restrictive subtype) | Stimulants, caffeine, nicotine | 10–15% |
The overlap is highest where impulsivity and binge-purge behaviour are already part of the eating disorder. Restrictive anorexia carries lower substance use rates overall, but a noteworthy pattern of stimulant and nicotine use specifically aimed at appetite suppression. This is part of what makes assessment difficult — the substance use can be a tool of the eating disorder, and the eating disorder can be a tool of the substance use.

Why Do These Two Conditions Travel Together?
Eating disorders and substance use disorders co-travel because they share the same brain reward circuitry, the same coping function, and often the same underlying distress. Both involve dysregulation of the dopamine and opioid reward systems, both serve as ways to manage difficult emotions, and both give the person a sense of control when other parts of life feel uncontrollable (Schreiber et al., Journal of Behavioral Addictions, 2013).
Three mechanisms explain why these conditions keep showing up together:
Shared reward biology. Brain imaging shows reduced availability of dopamine D2 receptors in the striatum of people with binge eating disorder, the same pattern seen in long-term stimulant and alcohol use. The reward system has become hyper-responsive and harder to satisfy, which drives both repeated drug use and repeated binge-purge cycles.
Shared regulatory function. The substance and the eating disorder behaviour are both doing a job — usually numbing, controlling, or escaping a feeling that the person cannot otherwise tolerate. Alcohol and food restriction can both produce dissociation. Stimulants and purging can both produce a punishing, clearing rush. Take one away without replacing the function, and the other intensifies.
Shared underlying drivers. Trauma, anxiety, emotional dysregulation, and adverse childhood experiences raise the risk of both eating disorders and substance use disorders independently, and raise the risk of having both together more than either alone (SAMHSA, 2026). This is why integrated treatment matters: the same therapeutic work — emotion regulation, distress tolerance, trauma processing — chips away at both conditions at once.

Why Does Treating the Addiction First Usually Fail?
“Get sober first, then deal with the eating disorder” sounds reasonable and is almost always wrong. The eating disorder is performing a regulatory function the substance used to share; when the substance is removed, the eating disorder behaviour intensifies to fill the gap. Early sobriety is often when bulimia, binge eating, and restrictive patterns get worse, not better — and that is when the relapse risk back to the substance is highest.
This is well documented in the clinical literature. People entering substance use treatment with active eating disorder symptoms tend to have worse substance use outcomes, more frequent relapses, and higher dropout rates than those without an eating disorder, particularly when the eating disorder is not addressed during the same treatment episode (Harrop and Marlatt, Addictive Behaviors, 2010).
What we see in practice maps onto the research:
- Alcohol detox without eating disorder support. Within days of last drink, bingeing on sugar and refined carbohydrates often surges as a substitute reward. For someone with bulimia, this can trigger a full relapse of binge-purge behaviour.
- Stimulant withdrawal without eating disorder support. Sleep collapses, appetite returns hard, and weight gain is rapid. For someone using stimulants partly for appetite suppression, this is the moment they reach for restriction or purging — and often the moment they reach back for the drug.
- Standard residential addiction treatment with three big meals and snacks. Without explicit meal planning, structure, and supervision tailored to the eating disorder, the food environment alone destabilises the client.
The sequential model survives because most addiction treatment centres are not staffed to treat eating disorders and most eating disorder services are not equipped to manage active substance use. Clients fall between the two systems. Integrated treatment exists to close that gap — when the clinical picture allows it.
The eating disorder is doing a job for the person. When we take the substance away, that job becomes more important, not less. If the eating disorder is medically safe enough to treat in a residential setting, treating both at once is almost always better than waiting. If it is not safe — if there is severe purging, electrolyte instability, or a dangerously low weight — we say so honestly, refer to a specialised eating disorder unit, and treat the addiction once the medical risk is contained.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
When Is Integrated Residential Treatment Appropriate?
Integrated residential treatment is appropriate when the eating disorder is moderate, the person is medically stable, and weight or electrolyte balance is not at acute risk. The substance use needs to be the more immediate threat, the eating disorder needs to be a co-existing condition that can be safely managed at residential level, and the person needs to be physically well enough to participate in a full treatment programme.
In practical terms, integrated treatment fits when:
- The eating disorder is bulimia nervosa or binge eating disorder without severe medical complications.
- The eating disorder is partly weight-restored anorexia with stable vitals and no need for tube feeding.
- Electrolytes, ECG, liver function, and kidney function are within a range the consultant psychiatrist and visiting medical doctor consider safe for residential care.
- The substance use is the more urgent presenting problem — alcohol dependence, stimulant misuse, or polysubstance use — and the eating disorder is a chronic background condition rather than an acute medical emergency.
- The person can eat meals with staff support, even if it feels difficult, without requiring locked-unit-level intervention.
The UK’s clinical guidance on eating disorders supports this approach. NICE recommends eating-disorder-focused cognitive behavioural therapy (CBT-ED, of which CBT-E is the dominant version) as a first-line psychological treatment for adults with bulimia nervosa, binge eating disorder, and many cases of anorexia, and there is consistent evidence that CBT-E can be adapted to integrate addiction-focused CBT when both conditions are present (NICE NG69, 2017; Sysko and Hildebrandt, European Eating Disorders Review, 2009).
Not sure whether your situation needs integrated treatment or a specialised eating disorder unit first? Talk to our admissions team — we will assess honestly and tell you if somewhere else would serve you better.
When Is One Step the Wrong Setting?
Integrated residential addiction and eating disorder treatment is the wrong setting when the eating disorder is medically dangerous on its own. A specialised eating disorder unit — with locked-unit capacity, dietitian-led tube feeding, refeeding syndrome monitoring, and continuous nursing cover — needs to come first. Once the person is medically stabilised and weight-restored to a safe level, integrated addiction and eating disorder work can begin in a residential setting like ours.
We do not take clients at One Step when any of the following are present:
- Dangerously low BMI requiring weight restoration as the primary treatment goal. NICE guidance on inpatient eating disorder care prioritises medical stabilisation and supervised refeeding, which we do not provide.
- Need for nasogastric tube feeding or any form of involuntary nutritional support.
- Severe purging with electrolyte derangement — low potassium, low sodium, abnormal ECG — that requires daily bloods and cardiac monitoring.
- Refeeding syndrome risk requiring careful nutritional reintroduction under specialist dietetic supervision.
- Active psychiatric crisis — acute suicidality, psychosis, or compulsory treatment orders. We are not a locked psychiatric facility.
These cases need a specialised eating disorder unit or a general psychiatric hospital first. We are happy to talk these decisions through with families, and where it is clear we are not the right fit, we will say so before any deposit is taken. The compass we use is whether the medical risk can be safely managed in a residential rehab setting — not whether we want the admission.

What Does Integrated Treatment Look Like at One Step?
For clients whose eating disorder is stable enough for residential care, One Step provides an integrated treatment plan built around shared case formulation, CBT-E running alongside addiction-focused CBT, supervised meals with clinical staff, and body image and emotion regulation work drawn from DBT. The eating disorder and the substance use are treated as connected problems with shared therapeutic targets, not as two separate conditions seen by two separate teams.
The practical elements:
- Shared case formulation. Our consultant psychiatrist, the assigned counsellor, and the visiting medical doctor build a single treatment plan that names how the eating disorder and the substance use are reinforcing each other for this specific client. Goals are co-set across both conditions.
- CBT-E integrated with addiction-focused CBT. CBT-E targets the over-evaluation of weight, shape, and eating that maintains the eating disorder. Addiction-focused CBT targets the cue-craving-use cycle. Sessions cross-reference each other rather than running in parallel silos. Our explainer on CBT and DBT for addiction covers how these therapies complement each other.
- Supervised meals. Meals are taken with clinical staff present, with portion structure, no skipping, and post-meal support to prevent purging and to sit with discomfort. This is part of the treatment, not just food.
- DBT for body image and distress tolerance. Dialectical behaviour therapy skills — distress tolerance, emotion regulation, opposite action — are used to manage the body image distress, restriction urges, and binge-purge urges that surface in early recovery.
- Family work where relevant. For adolescent-onset eating disorders and substance use, the family system often holds part of the problem. We include family sessions when the client agrees and family members are accessible, drawing on our family programme.
- Medical oversight from our consultant psychiatrist and visiting medical doctor. Regular medical check-ins, vitals, and review of any prescribed medication. For dual diagnosis where psychiatric medication is part of the plan, this links into our broader dual diagnosis programme.
The day-to-day setting is the same residential programme any other client would experience, with breakfast at 8, group therapy in the morning, individual sessions and skills groups through the afternoon, and supervised meals at fixed times. The treatment schedule sets the rhythm. The integrated work shows up in the content of the sessions, the meal supervision, and the shared case formulation behind the scenes.

Cost, Length of Stay, and What’s Included
The residential programme at One Step costs ฿280,000 per month (approximately USD 8,500). For clients with an eating disorder alongside substance use, most stays sit at the longer end of our 28-to-60-day range, because both conditions need time to stabilise and the integrated work takes longer than addiction treatment alone. Some clients stay 90 days when the eating disorder is more entrenched.
The fee covers accommodation in a private room, all therapy sessions and groups, supervised meals and snacks prepared on-site, intake assessment with our consultant psychiatrist, and the structured residential programme. Full details are on the pricing page.
The fee does not include medication prescribed by the doctor — refills of existing psychiatric or eating disorder medication, any newly prescribed drugs, and supplements are billed separately. It also excludes flights, visas, hospital visits, additional counselling sessions beyond the standard programme, and personal items. For the full exclusion list, see the pricing page.
If you want broader context on how dual diagnosis presentations are personalised in our programme, our posts on personalised dual diagnosis therapy options and the types of dual diagnosis therapies we use go into more detail.
Frequently Asked Questions
Common questions about dual diagnosis residential treatment for eating disorders and substance use.
It depends on your medical status. If your BMI is in a range the consultant psychiatrist considers safe for residential treatment, your vitals and electrolytes are stable, and you do not need tube feeding or daily medical monitoring, we can treat both conditions together. If you are at a dangerously low weight or need weight restoration as your primary goal, a specialised eating disorder unit needs to come first.
Because alcohol was doing some of the work your eating disorder behaviours also do — numbing, escaping, regulating mood. When alcohol is removed, the eating disorder steps in to fill that regulatory gap. Bingeing, restricting, and purging often intensify in the first weeks of sobriety. Treating both at once prevents this rebound from undoing the early sobriety work.
Stimulants do not cause eating disorders on their own, but they reinforce restrictive patterns and can entrench an existing eating disorder. Cocaine, methamphetamine, and prescribed stimulants like Adderall all suppress appetite, and many people with disordered eating use them partly for that reason. When stimulant use stops, appetite returns sharply — which is often the moment the eating disorder relapses or the person reaches back for the drug.
CBT-E (enhanced cognitive behavioural therapy) is a version of CBT designed specifically for eating disorders. It targets the over-evaluation of weight, shape, and eating control that maintains the disorder, and is recommended as a first-line treatment for bulimia, binge eating disorder, and many cases of anorexia by NICE. Standard addiction-focused CBT targets cravings, triggers, and the use cycle. At One Step we run both, integrated.
Our meals are prepared on-site with portion structure, taken with clinical staff supervision, and supported by post-meal sessions. We do not run a dedicated dietitian-led weight restoration programme and we do not provide nasogastric tube feeding. Clients who need weight restoration as the primary treatment goal need a specialised eating disorder unit first. We focus on stabilising eating patterns alongside addiction work.
Most clients with a co-occurring eating disorder and substance use disorder stay 60 to 90 days. The 28-day option some clients use for addiction alone is rarely enough when an eating disorder is also active — both conditions need time to stabilise, and the integrated therapeutic work takes longer than addiction treatment in isolation. Aftercare planning, including outpatient eating disorder therapy back home, is part of the discharge.
No. Medication is billed separately — you pay for what the consultant psychiatrist prescribes, plus any refills of existing prescriptions and supplements. This is the same for psychiatric medication, eating disorder medication, and any other drugs needed during your stay. The programme fee pays for the residential treatment itself; medication is billed separately, alongside flights, visas, and personal items.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








