
Key Takeaways
- Combining opioids and benzodiazepines is one of the most dangerous mixes in addiction medicine: each drug suppresses the brainstem signals that drive breathing, and together they multiply that effect.
- A landmark BMJ study of 315,428 patients found concurrent opioid and benzodiazepine use roughly doubled the risk of an overdose-related hospital visit (adjusted odds ratio 2.14).
- In 2016 the FDA put its strongest warning — a boxed warning — on around 400 opioid and benzodiazepine products specifically because of this combination.
- Quitting both cold turkey is dangerous in the opposite direction: benzodiazepine withdrawal can cause seizures and death, while opioid withdrawal is brutal but rarely lethal in otherwise healthy adults.
- The standard treatment approach is sequenced, not simultaneous: typically stabilise the opioid use first (often with medication), then taper the benzodiazepine slowly over months under medical supervision.
Opioids and benzodiazepines depress breathing through two different brainstem pathways, and combining them is what kills people. The U.S. FDA put its strongest warning label on this combination in 2016 after data showed the overdose risk roughly doubles when both drugs are on board (Sun et al., BMJ, 2017). This post covers why the combination is so lethal, why people end up on it (often without realising), and how withdrawal has to be managed when someone is dependent on both.
Why Are Opioids and Benzodiazepines So Dangerous Together?
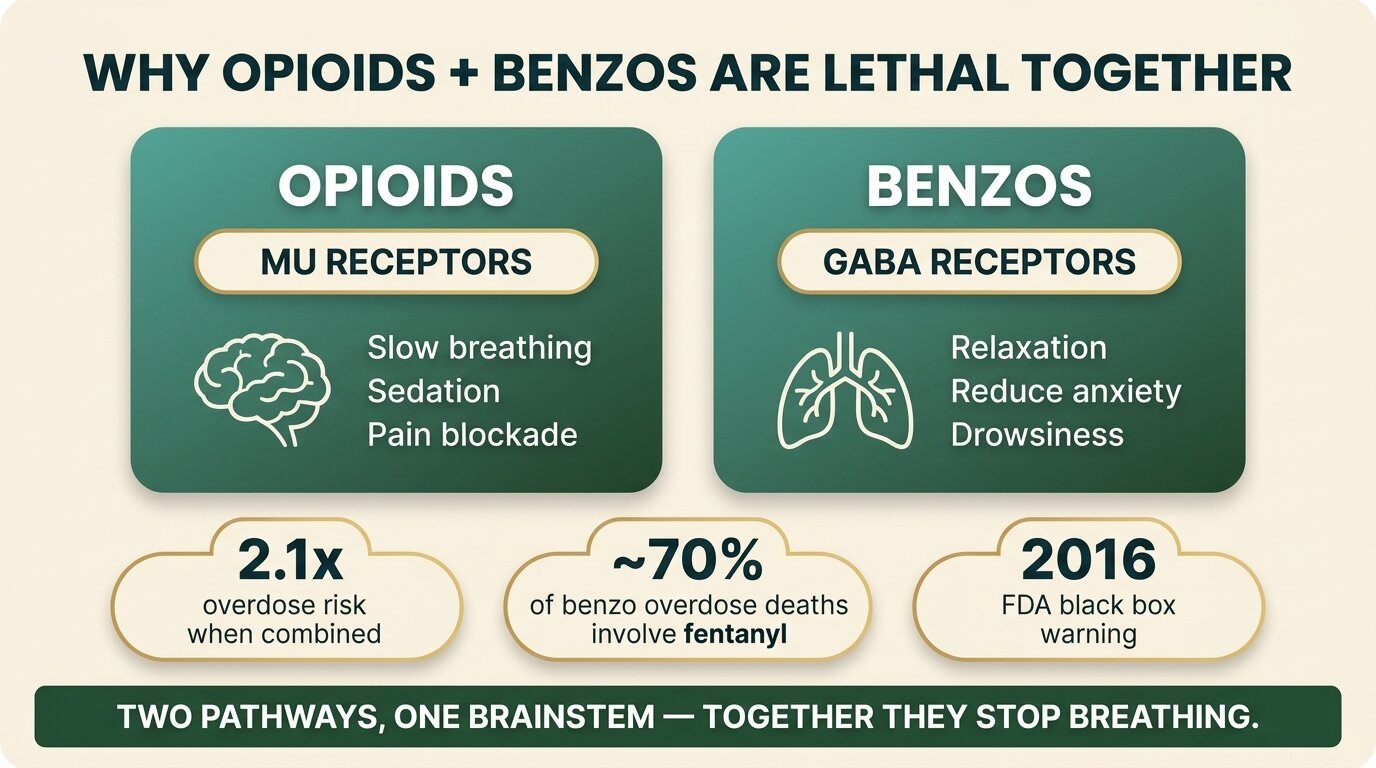
Opioids and benzodiazepines are dangerous together because they both shut down the brainstem signals that keep you breathing — but through different mechanisms. Opioids act on mu-opioid receptors in respiratory control areas like the preBötzinger complex. Benzodiazepines act on GABA receptors throughout the same brainstem network. When both drugs hit at once, the effects don’t just add — they amplify each other.
In plain English: your brain stem is what tells your lungs to breathe while you sleep. Opioids alone can dial that signal down. Benzodiazepines alone can dial it down. Take them together and the signal can drop low enough that you simply stop breathing — usually without any dramatic warning. This is why most fatal overdoses involving the combination happen during or just after sleep (Baertsch et al., eLife, 2021).
The FDA’s 2016 boxed warning — the strongest label warning the agency can require — was added to roughly 400 opioid and benzodiazepine products after years of overdose data made the risk impossible to ignore. The labels now state that combining the two can cause “profound sedation, respiratory depression, coma, and death.”
What Does the Overdose Data Actually Show?
The Sun et al. 2017 BMJ study tracked 315,428 insured patients prescribed opioids between 2001 and 2013 and found that concurrent benzodiazepine use roughly doubled the risk of an opioid-overdose-related emergency visit or hospital admission (adjusted odds ratio 2.14). The researchers estimated that eliminating concurrent use would cut overdose-related visits by about 15%.
The picture from death-certificate data is even starker. NIDA reports that benzodiazepine co-involvement in opioid overdose deaths climbed from 9% in 1999 to 21% in 2017, and that the large majority of all benzodiazepine-involved overdose deaths — over 80% — also involve an opioid (NIDA, 2024). More recently, the fentanyl era has changed the texture of the risk: in 2023, nearly 70% of overdose deaths involving benzodiazepines also involved illicitly manufactured fentanyl.
| Scenario | Overdose risk profile | What the evidence says |
|---|---|---|
| Opioid alone (prescribed, stable dose) | Baseline | Reference group in Sun et al. BMJ 2017 |
| Opioid + intermittent benzodiazepine | ~1.4x baseline | Adjusted OR 1.42 (Sun et al., 2017) |
| Opioid + chronic benzodiazepine | ~2.1x baseline | Adjusted OR 2.14 (Sun et al., 2017) |
| Illicit opioid (e.g. street fentanyl) + benzo | Substantially higher; unpredictable | ~70% of benzo-involved deaths in 2023 also involved fentanyl (NIDA, 2024) |

How Do People End Up Taking Both?
Most people on both drugs didn’t set out to mix them. The combination usually emerges from one of three patterns: a chronic pain prescription overlapping with an anxiety or sleep prescription written by a different doctor; deliberate use to amplify or extend an opioid high; or self-medication, where someone on opioids reaches for a benzodiazepine to manage the anxiety and insomnia that opioid use itself often produces.
The prescription-overlap pattern is the one that fooled the medical system for decades. A pain clinic writes oxycodone for a back injury. A psychiatrist writes alprazolam (Xanax) for generalised anxiety. Each prescriber knows their own piece. Neither sees the other’s notes. The patient takes them as prescribed and ends up in the highest-risk bracket without ever picking up an illegal drug. The 2016 FDA action was largely aimed at this exact gap.
The deliberate-combination pattern shows up most often with heroin or street fentanyl plus alprazolam or diazepam. Users describe it as “smoothing out” the opioid or extending the nod. From a brainstem-physiology standpoint, what they’re actually doing is layering two breathing-suppressants on top of each other — which is why this pattern accounts for so many fatal overdoses.
The self-medication pattern is the most subtle. Long-term opioid use frequently disrupts sleep, increases anxiety, and produces a low-grade restlessness that opioid prescribers don’t always recognise. A patient asks for “something to help me sleep,” gets a benzodiazepine prescription, and now the two drugs are layered without anyone calling it polysubstance use.
Why Is “Xanax for Anxiety, Oxy for My Back” a Clinical Landmine?
It’s a landmine because the patient often doesn’t see themselves as having a substance-use problem at all — both prescriptions are legal, both are taken as directed, and neither doctor flagged the combination. But the brainstem doesn’t care whether the drugs came from a pharmacy or a dealer. The risk of fatal respiratory depression is set by what’s in the bloodstream, not by who wrote the prescription.
Several real-world features make this scenario especially hard to catch:
- Different specialists, different records. Pain medicine and psychiatry are often in separate health systems. Before unified prescription drug monitoring programs, neither prescriber had any reliable way to see the other’s scripts.
- The patient doesn’t volunteer the information. Many patients assume the pain doctor doesn’t need to know about their anxiety medication, or vice versa. Some worry that disclosing the combination will get one of their prescriptions cut.
- Tolerance hides the danger. Someone who has been on a stable dose of both drugs for years can feel fine — right up until a new medication, an illness, alcohol, or a missed meal tips the balance and the same dose becomes lethal.
- Dose escalation creeps. Both classes lose effect over time. A patient who started on 5 mg of oxycodone and 0.25 mg of alprazolam years ago can quietly drift to several times that dose without any single appointment looking concerning.
The clinical literature is unambiguous about what should happen when this combination is identified. The American Society of Addiction Medicine’s 2025 joint clinical practice guideline on benzodiazepine tapering specifically calls for more frequent risk-benefit reassessment whenever a patient is taking both classes, and discourages routine long-term co-prescription unless clearly necessary and tightly monitored (ASAM, 2025).
The patient who scares me most is not the person buying street drugs — it’s the middle-aged professional on a stable oxycodone prescription for a back injury and a stable alprazolam prescription for panic attacks. Both doses look reasonable on paper. Neither doctor has done anything wrong. But the breathing risk is the same as anyone else mixing the two, and these patients often die in their sleep before anyone realises they had a problem.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
If you’re taking both a prescribed opioid and a prescribed benzodiazepine — or you’re worried about a family member who is — talk to our team. We’ll give you a straight read on whether residential treatment is the right next step.
How Is Withdrawal Managed When Someone Is Dependent on Both?
Withdrawal from both drugs is not symmetrical and cannot be treated symmetrically. Benzodiazepine withdrawal can cause seizures and is occasionally fatal, while opioid withdrawal is severe but rarely life-threatening on its own. Because of that asymmetry, the standard approach is to stabilise the opioid component first — usually with medication — then taper the benzodiazepine slowly under medical supervision. Stopping both at once is dangerous in a way that frightens experienced clinicians.
The general sequencing logic looks like this:
- Medical assessment first. Doses, duration, last use, prior withdrawal seizures, mental-health history, and any cardiac or respiratory illness all feed the plan. Severe dependence on either drug — particularly benzodiazepines — usually triggers a hospital-based detox before residential rehab.
- Stabilise the opioid. For most clients with significant opioid dependence, this means starting medication for opioid use disorder (typically buprenorphine or methadone) rather than trying to push through cold-turkey opioid withdrawal while a benzodiazepine taper is in progress.
- Begin a slow benzodiazepine taper. The 2025 ASAM joint clinical practice guideline recommends an initial pace of roughly 5-10% of the current dose every 2-4 weeks, with the taper typically not exceeding 25% every 2 weeks. Long-acting benzodiazepines like diazepam are often substituted for short-acting ones like alprazolam before the taper starts.
- Address sleep and anxiety with non-benzodiazepine tools. CBT for insomnia, trauma-focused therapy, and structured daily routines do most of the heavy lifting that the benzodiazepine used to do — without the respiratory risk.
- Plan for long timelines. A clinically appropriate benzodiazepine taper after years of use can take many months. Trying to compress it into a 28-day rehab stay is one of the most common reasons people relapse.
It’s worth being honest about a complication people don’t expect: the benzodiazepine taper is often the longest, slowest, most uncomfortable part of the whole process — long after the opioid side feels manageable. Patients who were sold the idea that “rehab fixes you in 28 days” often hit a wall around week three or four when they realise the benzodiazepine work is going to outlast their residential stay.

How Does One Step Handle Opioid + Benzodiazepine Dependence?
One Step Rehab in Chiang Mai treats opioid and benzodiazepine dependence, including the dual-dependence pattern described in this post — but the medical reality of severe benzodiazepine withdrawal means we don’t try to handle the highest-risk detoxes on-site. For those clients, we route the detox phase through our partner hospital first, then bring them into our 28-60 day residential programme once they’re medically stable.
The practical breakdown:
- For severe withdrawal, we may detox you first at our partner hospital — which has intensive and intermediary intensive care units — before you transfer to One Step for the rehab programme. This is the appropriate route for anyone with significant long-term benzodiazepine dependence combined with opioid use, prior withdrawal seizures, or serious medical comorbidities.
- For more moderate cases, particularly where the opioid side is the bigger issue and benzodiazepine use is short-term or low-dose, the detox and stabilisation can usually happen on-site at One Step under our medical team’s supervision.
- The residential programme runs ~฿280,000/month (~$8,500 USD) and includes individual and group therapy, our structured treatment programme, accommodation, food, and the day-to-day clinical support. Medication is billed separately — you pay for what the doctor prescribes, which for this client group typically includes buprenorphine or methadone for the opioid side and a long-acting benzodiazepine for the taper.
- Hospital-based detox, if needed, is also billed separately. The pricing page (see what’s included) lists hospital visits and detox at the partner hospital as items outside the programme fee.
- Realistic timelines. A benzodiazepine taper that’s safe to attempt — let alone complete — inside a residential stay is rare. Most clients in this category will leave residential treatment still on a slow taper, which we hand over to a prescriber in their home country with a clear plan in place.
If you’re calling us about a family member, the most important question we’ll ask is what they’re actually taking — drug name, dose, how long, and what else (alcohol, other sedatives, antidepressants) is in the picture. That information shapes whether the appropriate first step is residential rehab, hospital detox, or a slower outpatient taper before they ever travel.
Treatment for this kind of polysubstance pattern almost always continues after residential. We connect clients with prescribers and therapists for the long benzodiazepine taper, and our aftercare programme stays involved for the first year — the period during which relapse risk and overdose risk are both highest. For broader context on what residential treatment looks like, our inpatient vs outpatient comparison walks through who each option fits. Clients who arrive on benzodiazepines specifically should also read our benzodiazepine rehab page and our opioid rehab page for the substance-specific picture.
Frequently Asked Questions
Common questions about combined opioid and benzodiazepine use, withdrawal, and treatment.
Only with active prescriber coordination and at the lowest effective doses for the shortest duration. The FDA’s 2016 boxed warning explicitly tells doctors to avoid this combination unless alternative treatments have failed. If both prescribers know about each other and the combination is genuinely necessary, it can be done — but routine long-term co-prescription is exactly what the warning is trying to prevent.
Because benzodiazepines suppress the brain’s GABA system, and pulling them away too quickly can cause grand mal seizures, delirium, and occasionally death. Opioid withdrawal is brutally uncomfortable — vomiting, body aches, insomnia, anxiety — but in otherwise healthy adults it’s rarely lethal. That asymmetry is why protocols stabilise the opioid side first and taper the benzodiazepine slowly.
No — and any prescriber or rehab that suggests it is taking an unsafe shortcut. Stopping a benzodiazepine cold turkey after sustained use can cause seizures. Simultaneously stopping an opioid stacks severe withdrawal symptoms on top, which makes the seizure risk worse and almost guarantees relapse. Sequenced withdrawal under medical supervision is the established standard of care.
For someone on long-term benzodiazepines, the ASAM 2025 guideline recommends an initial pace of roughly 5-10% of the current dose every 2-4 weeks, not exceeding 25% every 2 weeks. For someone who’s been on a daily dose for years, that often translates to a taper measured in many months, not weeks. Faster tapers cause withdrawal symptoms that drive people back to the drug.
Both are medications used to stabilise opioid dependence so the patient isn’t fighting opioid withdrawal at the same time as the benzodiazepine taper. They reduce cravings, prevent withdrawal, and dramatically reduce overdose risk during the period when relapse is most likely. They’re not a substitute for therapy — they’re the medical floor that makes therapy possible.
Yes, and arguably worse. Street fentanyl is unpredictable in potency, so the “safe” dose moves around between batches. Add a benzodiazepine — increasingly, illicit ones like etizolam that aren’t reversed by standard treatments — and overdose risk climbs sharply. CDC data shows nearly 70% of benzodiazepine-involved overdose deaths in 2023 also involved illicit fentanyl.
Get naloxone (Narcan) in the house and learn how to use it — it can reverse the opioid side of an overdose long enough for an ambulance to arrive. Then have a calm, non-confrontational conversation about getting medical help for the combination, not just one drug. Most fatal overdoses involving this mix happen during sleep, so the household safety piece is genuinely life-saving.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








