Key Takeaways
- There is no single “dual diagnosis programme” — what matters is a plan built for the specific combination of substance and psychiatric condition. Treating depression with someone in active alcohol withdrawal looks nothing like treating PTSD in a stable cocaine recovery.
- The “treat the addiction first, then the mental health” model fails because untreated psychiatric symptoms drive relapse, and unmanaged substance use prevents psychiatric medication from working. SAMHSA and NIDA both recommend integrated treatment — both conditions, same team, same time.
- At One Step, personalisation means a clinician-led case formulation in the first week, weekly plan adjustments, and a therapist mix matched to the diagnosis: CBT and DBT for mood and emotion regulation, EMDR and trauma-focused work for PTSD, behavioural activation for depression, exposure work for anxiety.
- Medication management is handled by a visiting consultant psychiatrist — Dr. Worapakthorn — who assesses, prescribes, and adjusts during the stay. Medication itself is billed separately from the programme fee.
- Some cases need a higher level of care than residential rehab can provide: active psychosis, acute suicidal crisis, severe bipolar mania, eating disorders requiring NG-tube feeding. We will tell you upfront if that applies.
Personalised dual diagnosis therapy is not a single programme — it is a treatment plan adapted to the specific combination of substance use disorder and co-occurring mental health condition you arrive with. Someone in alcohol withdrawal with severe depression needs a different first week than someone with stable cocaine recovery and PTSD. SAMHSA’s updated guidance is explicit: integrated treatment — both disorders, same team, same time — produces better outcomes than treating one disorder and then referring the person elsewhere for the other (SAMHSA TIP 42, 2020).
What Does “Personalised Dual Diagnosis Therapy” Actually Mean?
Personalised dual diagnosis therapy means a treatment plan built from your specific case — the substance, the psychiatric diagnosis, the symptom severity, the trauma history, the medication picture — rather than slotting you into a generic timetable. At One Step, a consultant psychiatrist and senior therapist build the plan in the first week, then adjust it weekly as symptoms shift.
The word “personalised” is overused in rehab marketing. In practice, it should mean three concrete things: (1) a documented case formulation done by clinicians, not a salesperson; (2) therapy modalities chosen for your diagnoses, not a fixed weekly schedule everyone follows; (3) explicit decision points where the plan is reviewed and changed if something is not working.
If a facility tells you their programme is “personalised” but everyone does the same group therapy on the same day at the same time, the personalisation is cosmetic. Real personalisation looks like: an EMDR slot replacing a CBT slot once a trauma assessment confirms PTSD; a medication switch from an SSRI to a different antidepressant after two weeks of poor response; a step-up in family work when the family system is identified as a relapse driver.
Why Doesn’t “Treat the Addiction First, Then the Depression” Work?
Treating substance use first and mental health second fails because the two disorders drive each other. Untreated depression, anxiety, or PTSD is one of the strongest predictors of relapse during early recovery. And active substance use blocks psychiatric medication from doing its job. Integrated treatment — addressing both together — is now the standard of care (NIDA, 2024).
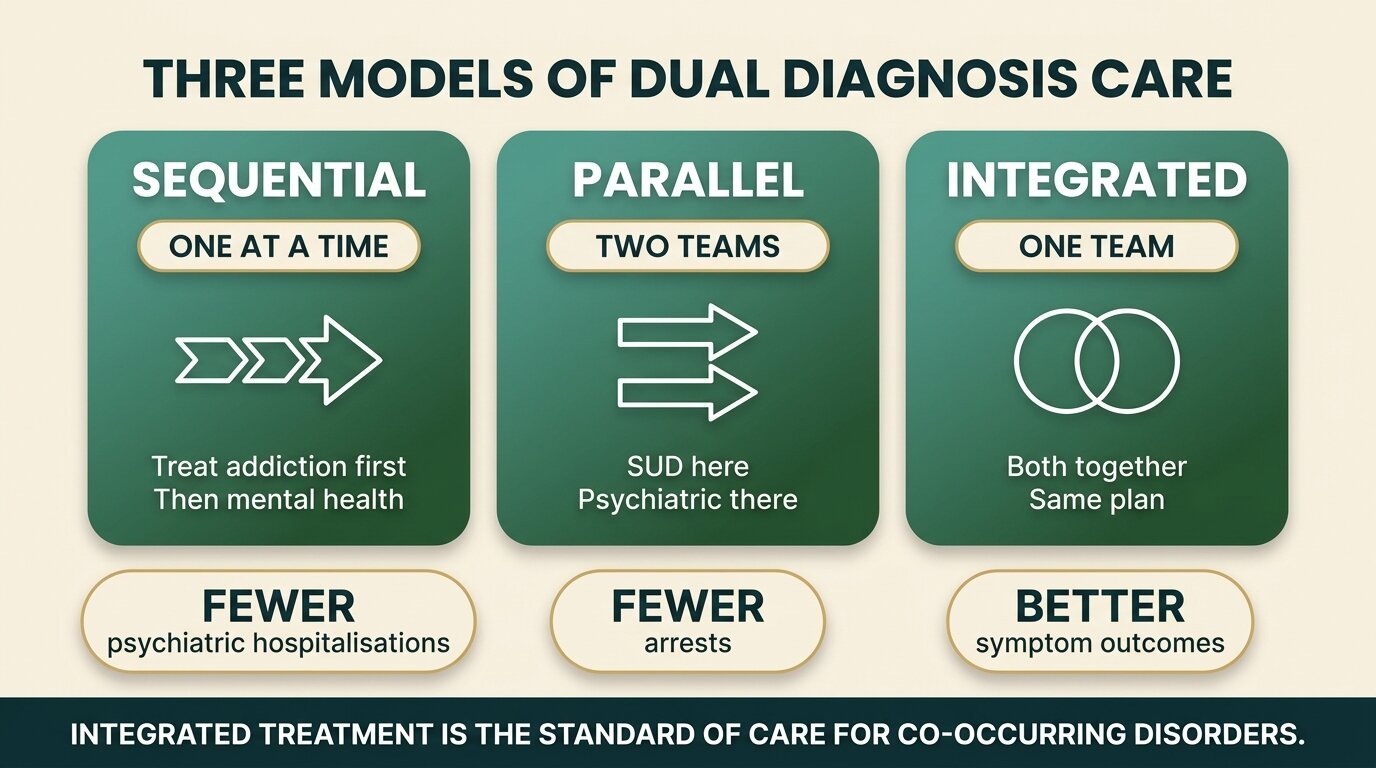
The older model was sequential: detox the person, complete a substance use programme, then refer them on to a psychiatric service for the depression or PTSD. The problem is that the gap between programmes is exactly when relapse happens. The depression that drove the drinking is still there at week six of sobriety, and the person now has no structure and no clinical support.
The parallel model is slightly better — substance use treatment in one building, psychiatric care in another, two separate teams who do not talk. It still fails the basics of integrated care: no shared treatment plan, no shared progress notes, no single clinician with the whole picture.
Integrated treatment puts both disorders under one clinical team with one plan. A 216-person comparison found that the integrated group had significantly fewer psychiatric hospitalisations and arrests than the parallel-treated group (Mangrum et al., J Subst Abuse Treat, 2006). A 2023 systematic review confirmed that integrated treatment produces better psychiatric symptom outcomes, though the substance use outcomes are similar — meaning the addiction work itself is solid in both, but the mental health side only properly resolves under the integrated model (Chetty et al., Health SA, 2023).
Which Combinations of Diagnoses Does One Step Actually Treat?
One Step treats substance use disorders that co-occur with depression, anxiety disorders, PTSD and complex trauma, bipolar II (in a stable phase), and ADHD. The treatment plan is built around the specific combination — there is no generic “dual diagnosis” track. Some severe presentations need a higher level of care first; those cases are flagged at assessment.
The most common combinations we see in residential treatment are alcohol use disorder with depression, cocaine use disorder with anxiety, and any substance use disorder with PTSD or trauma. These respond well to integrated residential work because the structure of inpatient care — set wake times, no substances available, daily therapy — is itself part of the depression and anxiety treatment.
What we will tell you upfront we cannot fully manage: active psychosis (requires hospital first), acute suicidal crisis with intent and plan (requires hospital first), severe bipolar mania in an acute episode, and eating disorders requiring nasogastric tube feeding. We are not a locked psychiatric facility — for those situations, hospitalisation is the safer first step, and we can take the client afterwards once the acute phase is stabilised.
| Combination | Primary therapy mix | Medication picture |
|---|---|---|
| Alcohol use disorder + depression | CBT, behavioural activation, relapse prevention work, exercise structure | SSRI started after detox stabilises, reviewed at 2 and 4 weeks |
| Cocaine use disorder + anxiety | CBT for anxiety, mindfulness skills, urge management, sleep work | Non-benzodiazepine options reviewed; benzos avoided where possible |
| Any SUD + PTSD / complex trauma | Stabilisation phase first, then EMDR or trauma-focused CBT, somatic skills | SSRI / SNRI as standard; prazosin for nightmares where appropriate |
| SUD + bipolar II (stable) | Psychoeducation, mood charting, sleep and routine work, DBT skills | Mood stabiliser maintained or reviewed; close psychiatric oversight |
| SUD + ADHD | Structure-heavy programme, behavioural skills, often referred for psychometric assessment | Stimulant decisions made cautiously and only after stable abstinence |

Which Therapies Do You Actually Use at One Step?
At One Step the working therapy mix is CBT (cognitive behavioural therapy), DBT (dialectical behaviour therapy), EMDR for trauma, trauma-focused CBT, behavioural activation for depression, exposure-based work for anxiety, motivational interviewing, and family systems work. The mix per client is selected by the lead therapist after assessment, not assigned to everyone by default.
CBT and DBT each do a different job in dual diagnosis. CBT targets the thought-behaviour loop — the catastrophic thinking that drives the drinking, the avoidance that keeps anxiety alive. DBT targets emotion regulation when the underlying problem is that feelings escalate too fast to manage without using. Most clients get elements of both; the proportion shifts depending on diagnosis. We unpack the difference in detail in our breakdown of CBT vs DBT for addiction.
EMDR (Eye Movement Desensitisation and Reprocessing) is the trauma modality with the strongest evidence base for PTSD. We do not start EMDR in the first week — the client needs to be stable, sober, sleeping, and grounded before trauma reprocessing begins. Trying to do trauma work too early is one of the classic mistakes in dual diagnosis treatment.
Behavioural activation is the workhorse for depression — getting the client doing things again, in scheduled small steps, before the mood is ready. Exposure work for anxiety follows the same logic: structured, graded, with the therapist alongside. Both are delivered by individual therapists, not in group settings.
The mistake I see most often in dual diagnosis is the assumption that one diagnosis is the “real” problem and the other is downstream. In practice, you have to treat both as primary. If you wait for depression to lift before doing substance use work, it will not lift. If you wait for abstinence to settle before treating PTSD, the client will relapse to manage the trauma symptoms. The plan has to address both from week one — only the intensity and sequencing changes as the person stabilises.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab

How Is Psychiatric Medication Managed During the Stay?
Psychiatric medication is managed by Dr. Worapakthorn, our consultant psychiatrist, who assesses every client during intake, prescribes or adjusts medication during the stay, and reviews progress at set checkpoints. Existing prescriptions are continued and reviewed; new medication is started when clinically indicated. The medication itself is billed separately from the programme fee.
The intake assessment covers current medication, past psychiatric history, what has been tried before, and what has worked or failed. For most clients, the first decision is whether to continue an existing antidepressant, switch it, or wait until the substance use has been stable for a few weeks before evaluating. Restarting medication during active withdrawal is rarely useful — the symptoms overlap and you cannot tell what is working.
Medication changes happen on a clinical timeline, not a programme timeline. An SSRI typically takes four to six weeks to show full effect. Mood stabilisers need lab monitoring. ADHD stimulant decisions, in particular, are made cautiously in early recovery — the same reward system that responds to a stimulant prescription was just disrupted by the substance use.
One honest note about cost: medication is billed separately — you pay for what the doctor prescribes during your stay, the same way you would pay for medication at home. The pricing page lays out exactly what is and is not covered in the programme fee.
Not sure whether residential dual diagnosis treatment is the right level of care for your situation? Talk to our team — we will tell you straight, including if we think a different setting would serve you better.
What Does Personalisation Actually Look Like Week by Week?
Personalisation at One Step is a structured process: psychiatric assessment in week one, individual case formulation written by the lead therapist, a weekly clinical review where the plan is adjusted, and a discharge plan built around the client’s specific risk profile rather than a template. The same client at week four will be on a different schedule from week one.
Week one is assessment-heavy. The consultant psychiatrist meets the client. The lead therapist meets the client. A formulation is drafted — what the diagnoses are, what the drivers are, what the goals are, what therapies are indicated. This formulation is the document the rest of the treatment runs off.
From week two, individual therapy sessions are matched to the formulation. A client with PTSD will be doing stabilisation work and starting EMDR by week three or four. A client with depression will be doing behavioural activation and CBT. A client with bipolar II will have heavy psychoeducation and mood monitoring. Group work continues across all clients — relapse prevention, process group, life skills — because the shared community piece is therapeutic in itself. The full treatment schedule shows how individual and group sessions sit alongside each other in the day.
Weekly clinical reviews are where personalisation lives or dies. The team meets, looks at how the client is responding, and changes the plan if it is not working. That can mean adding sessions, dropping sessions, switching therapists, adjusting medication, or bringing family into the work. Without these reviews, “personalised” is just a brochure word.
Family work is offered where the family system is part of the picture — and most of the time, it is. We run video calls and structured family sessions when the client and family consent. Where the family is the relapse driver, the work is heavier; where the family is supportive, it is lighter. The family programme explains what is involved.
How Does One Step Run Dual Diagnosis Treatment Day to Day?
One Step is a residential treatment centre in Chiang Mai running structured 28-day-and-up programmes. The fee is approximately ฿280,000/month (around $8,500 USD). The day has set times — wake, group therapy, individual sessions, meals, activities, evening reflection. Dual diagnosis clients follow the same structural day with individual sessions and medication oversight built around their specific plan.
The client mix matters in residential dual diagnosis. We keep the resident group small — most clients are working through some combination of substance use plus mental health concern, so the group itself is more accepting of psychiatric content than a substance-only setting would be. Group sessions cover relapse prevention, communication skills, and process work; nobody is excluded from group for having a mental health diagnosis.
Detox, when needed, happens on site for most cases — alcohol, cocaine, ketamine, methamphetamine, cannabis, most opioid presentations. For severe alcohol or benzodiazepine withdrawal, we may detox you first at our partner hospital — which has intensive and intermediary intensive care units — then you transfer to One Step for the rehab programme. Our guide to inpatient vs outpatient rehab explains why the residential structure matters for dual diagnosis specifically.
For broader context on how we approach co-occurring conditions across the programme, our dual diagnosis treatment page covers the clinical structure in more detail. Aftercare planning starts before discharge — the relapse risk in early dual diagnosis recovery is high, and the handover to ongoing psychiatric and counselling support has to be specific, not vague. Our aftercare programme covers the post-discharge structure.
What is included in the fee: accommodation, meals, group therapy, individual therapy sessions, group activities, intake psychiatric assessment and routine progress checks. What is not included: medication prescribed during the stay, flights, visas, supplements, additional counselling sessions beyond the programme allocation, hospital visits, and personal items. Full detail is on the pricing page.
If you or someone you love is struggling with substance dependence, explore how a drug addiction treatment in Thailand can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
What families and clients most often ask about personalised dual diagnosis therapy.
At One Step the programme fee is the same — approximately ฿280,000/month — whether you arrive with substance use alone or with a co-occurring mental health diagnosis. What changes is the therapy mix and the involvement of the consultant psychiatrist. Medication and any additional counselling sessions beyond the standard allocation are billed separately.
Most dual diagnosis clients stay 60 to 90 days rather than the 28-day minimum. The reason is clinical, not commercial: psychiatric medication often takes four to six weeks to show full effect, and trauma work cannot start until the client is stable. A 28-day stay rarely gives enough time to assess, stabilise, treat, and plan discharge for a complex case.
Yes, and we do — but with sequencing. The first two to three weeks focus on stabilisation: detox if needed, sleep restoration, grounding skills, daily structure. EMDR or other trauma-focused work begins once the client is sober, sleeping, and able to tolerate the material. Starting trauma reprocessing in early withdrawal makes symptoms worse, not better.
No. Existing psychiatric medication is reviewed at intake by Dr. Worapakthorn and continued unless there is a clinical reason to change. Stopping an SSRI abruptly during early recovery is usually a bad idea — the discontinuation symptoms layer on top of withdrawal and make everything worse. If a change is needed, it is done gradually with monitoring.
We treat bipolar II in a stable phase alongside substance use, with mood-stabilising medication oversight, mood charting, DBT skills, and structured routine. We are not the right setting for someone in an acute manic episode or severe mixed state — that needs hospital-level care first. Once the acute phase is stabilised, we can take the client for the rehab work.
It is offered, not compulsory. Family work is included where the client consents and where the family system is part of the clinical picture — for example when family dynamics are a relapse driver, or when family support will be central to aftercare. We do this through structured video calls and, where geography allows, in-person sessions later in the stay.
We will tell you at the assessment stage. If someone is in active psychosis, an acute suicidal crisis, or a severe bipolar episode, hospital-level care has to come first — we are not a locked psychiatric facility and cannot manage acute crisis safely. Once the acute phase is stabilised by hospital care, we can take the client for the residential rehab work.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn