Key Takeaways
- Cannabis withdrawal is a real, recognised condition — formally added to the DSM-5 in 2013 after decades of dismissal.
- Roughly 47% of regular cannabis users experience meaningful withdrawal symptoms when they stop, rising to 87% in inpatient settings (Bahji et al., JAMA Netw Open, 2020).
- Symptoms peak between days 3 and 7 — sleep loss, irritability, anxiety, sweating, appetite loss, vivid dreams — and resolve over 2-3 weeks for most people.
- It is miserable but not life-threatening. No medical detox is required. Sleep disturbance and cue-triggered cravings can persist for months in heavy long-term users.
- What helps: structured days, exercise, sleep hygiene, and accountability. What doesn’t: white-knuckling alone or substituting alcohol.
Yes, cannabis withdrawal is real. The American Psychiatric Association added Cannabis Withdrawal as a formal diagnosis to the DSM-5 in 2013 (Hasin et al., Am J Psychiatry, 2013), and a 2020 meta-analysis of more than 23,500 users found roughly 47% of regular users experience meaningful withdrawal symptoms when they stop (Bahji et al., JAMA Netw Open, 2020). The “weed isn’t addictive” line you’ve heard for years is wrong. It’s not life-threatening like alcohol or benzodiazepine withdrawal — nobody seizes coming off cannabis — but it is genuinely unpleasant, and the timeline is predictable enough that you can plan around it.
This post walks through what happens day by day, what helps, what makes it worse, and how a structured residential setting like One Step handles cannabis discontinuation. If you’ve tried to quit before and gave up around day four when you couldn’t sleep, this is why.
Is Cannabis Withdrawal Actually Real?
Yes. Cannabis withdrawal is a recognised clinical syndrome in the DSM-5 since 2013, with seven defined symptoms including irritability, anxiety, sleep difficulty, decreased appetite, restlessness, depressed mood, and physical discomfort like sweating, tremor, or stomach pain. It affects roughly half of regular users and up to 87% of those in inpatient settings.
The reason “weed isn’t addictive” stuck around for so long is partly cultural and partly because the original DSM-IV in 1994 didn’t recognise cannabis withdrawal at all — there wasn’t enough research evidence at the time. That evidence accumulated over the next two decades. By 2013, researchers had documented a consistent symptom pattern across both controlled abstinence studies and clinical populations, and the diagnosis was added to the DSM-5 (Hasin et al., Am J Psychiatry, 2013).
What’s happening physically: heavy cannabis use down-regulates the brain’s CB1 cannabinoid receptors. When THC is suddenly removed, the endocannabinoid system is left in a state of relative deficit until receptors recover — which takes roughly four weeks of abstinence (Schlienz et al., Curr Addict Rep, 2017). That receptor rebound is what’s driving the irritability, anxiety, and sleep disruption you feel during the first month.
What Does the Cannabis Withdrawal Timeline Look Like Day by Day?
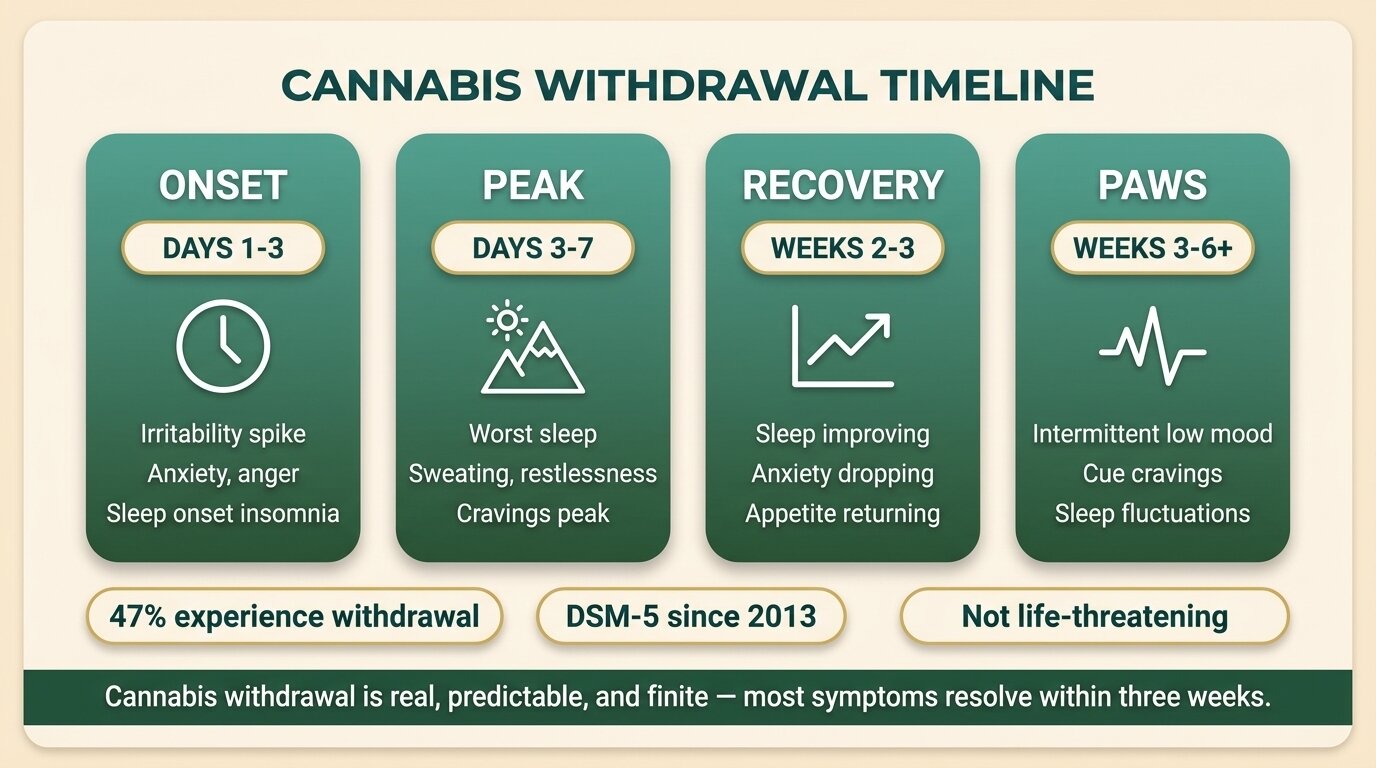
Cannabis withdrawal usually starts within 24-48 hours of last use, peaks between days 3 and 7, and resolves over 2-3 weeks for most people. The first phase is irritability and sleep onset insomnia. The peak brings the worst sleep, sweating, restlessness, and cravings. Then symptoms gradually improve, with sleep often the last thing to normalise.
| Phase | Timing | What you feel |
|---|---|---|
| Onset | Days 1-3 | Irritability spike, anxiety, anger, sleep onset insomnia, vivid dreams once REM rebounds |
| Peak | Days 3-7 | Worst sleep, sweating, restlessness, appetite loss, cravings peak, GI upset in some people |
| Resolution | Weeks 2-3 | Sleep slowly improves, anxiety baseline lowering, appetite returning |
| PAWS | Weeks 3-6+ | Intermittent low mood, sleep disturbance, cue-triggered cravings — can persist for months in heavy long-term users |
Days 1-3: The Irritability Spike
Most people notice the first symptoms 12-24 hours after their last use. The early signs are a sharp rise in irritability and anxiety, plus difficulty falling asleep. Anger can come out of nowhere — small things become outsized. Sleep onset insomnia is one of the most reliable early markers. Once you do fall asleep, vivid dreams kick in as REM sleep rebounds — your brain has been suppressing REM for as long as you’ve been using, and it catches up fast (Schlienz et al., Curr Addict Rep, 2017).
Days 3-7: The Peak
This is the worst window — and the point at which most people who try to quit on their own go back. Sleep collapses. You’ll wake repeatedly, sweat through sheets, and feel restless and physically uncomfortable in a way that’s hard to describe. Appetite drops. Cravings peak around day 4-5. Some people develop GI upset — nausea, stomach pain, loose stools. Onset is typically days 1-3, peak between days 2-6, and most effects last 4-14 days (Bonnet & Preuss, Subst Abuse Rehabil, 2017).
Weeks 2-3: Things Start Improving
By day 10-14, most acute symptoms are receding. Sleep is still disturbed but improving. The baseline anxiety drops noticeably. Appetite usually returns first — often with a rebound where everything tastes more intense than it has in years. Mood is still volatile but the sharp irritability of week one is gone.
Weeks 3-6+: PAWS (Post-Acute Withdrawal)
For heavy long-term users — people who’ve used daily for years — symptoms don’t fully resolve at three weeks. Sleep architecture continues to recover gradually, low mood comes and goes, and cue-triggered cravings (a specific smell, a song, walking past a particular spot) can hit hard months after the last use. This is normal and it does fade. Knowing it’s coming makes it easier to ride out.
What Symptoms Should You Actually Expect?
The most common cannabis withdrawal symptoms, in roughly descending frequency, are: sleep difficulty, irritability, anger or aggression, anxiety, restlessness, decreased appetite, depressed mood, and vivid or strange dreams. About a third of people also get physical symptoms — sweating, chills, headache, stomach pain, or tremor. Cravings are nearly universal in heavy users.
The DSM-5 diagnosis requires at least three symptoms appearing within a week of stopping heavy, prolonged use. The seven recognised symptoms are:
- Irritability, anger, or aggression — usually the first thing partners and family notice
- Nervousness or anxiety — a low-grade buzz that can spike into panic in heavy users
- Sleep difficulty — including vivid dreams and nightmares once REM rebounds
- Decreased appetite or weight loss — food loses appeal for days at a time
- Restlessness — physical inability to settle
- Depressed mood — flat, demotivated, “why bother”
- Physical symptoms — at least one of: stomach pain, shakiness, sweating, fever, chills, or headache
A residential study of 45 cannabis-dependent users tracking symptoms over 28 days found decreased appetite, sweating, and craving were the most consistent markers across the withdrawal period (Sharma et al., Eur Psychiatry, 2023). The takeaway: don’t trust internet lists that focus only on cravings. Sleep and irritability are bigger drivers of why people relapse during week one.
The reason cannabis withdrawal blindsides people is they don’t expect it. They’ve been told for years that weed isn’t physically addictive, so when they hit day four with no sleep, raging at their partner, and unable to eat, they assume something else is wrong. Naming it — telling them this is textbook cannabis withdrawal, here’s the timeline, here’s when it stops — takes most of the fear out of it.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab

Why Is Sleep the Hardest Part?
Sleep is the most disrupted and the slowest to recover system in cannabis withdrawal. Polysomnography studies show abrupt cannabis cessation reduces total sleep time and slow-wave sleep, increases time spent awake in bed, and triggers REM rebound — meaning more REM sleep with shorter REM latency, which produces vivid and often disturbing dreams. These changes begin from the first night of abstinence in heavy users.
If you’ve been using cannabis daily to fall asleep, your brain has been suppressing REM and slow-wave sleep for as long as you’ve been using. The first few nights without it are brutal: you can’t fall asleep, and when you do, your brain crams in a backlog of REM that produces intense, technicolour dreams — often nightmares. People describe waking up at 3am soaked in sweat and not sleeping again until dawn.
This is the single biggest reason people relapse in week one. We’ve written separately about why your sleep collapses when you stop a substance you’ve been using to sleep — the cannabis pattern follows the same shape as the alcohol pattern, with REM rebound being the most pronounced feature. Knowing this is happening and that it does end makes it easier to ride out. Skipping caffeine after noon, exercising in daylight hours, and getting up at the same time every day even when you’ve barely slept — these are the boring fundamentals that work.
Quitting cannabis on your own and getting stuck at the peak? Talk to our team — we’ll tell you honestly whether a residential stay is what you need or whether structured outpatient support would do it.
What Helps During Cannabis Withdrawal — and What Doesn’t?
What helps: a structured day with set wake and bed times, daily aerobic exercise, decent food when you can manage it, no caffeine after noon, and someone to be accountable to. What doesn’t: trying to white-knuckle it alone, switching to alcohol or other substances, doomscrolling at 3am when you can’t sleep, or using “just a little” to take the edge off — which resets the clock.
| Helps | Doesn’t help |
|---|---|
| Structured daily routine — same wake and bed times | Lying in bed all day waiting for it to pass |
| Daily aerobic exercise, ideally in daylight | Substituting alcohol or benzodiazepines to sleep |
| Sleep hygiene — no caffeine after noon, no screens in bed | Scrolling phone at 3am when you can’t sleep |
| Accountability — partner, sponsor, residential setting | Telling no one and trying to white-knuckle alone |
| Eating small meals even when not hungry | “Just one” hit to take the edge off — resets the clock |
| Knowing the timeline — peak ends, sleep returns | Catastrophising — “this is forever” |
The substitute-with-alcohol move is the most dangerous of these. We see it constantly: someone stops cannabis, can’t sleep, drinks themselves to sleep for a week, and now has an alcohol problem on top of the original cannabis problem. Alcohol withdrawal is far worse than cannabis withdrawal — it can kill you. Don’t trade one substance for another to get through the peak.
The other common trap is “just one.” A single use during day 4 or 5 doesn’t undo all your progress, but it does delay the receptor recovery and restart the symptom clock. You’ll get to day 7, feel the peak again, and probably use again. Most relapses follow this exact pattern. If you can get past day 7 fully clean, the rest gets easier.

Which Therapies Actually Work for Cannabis Use Disorder?
Cannabis use disorder responds best to a combination of cognitive behavioural therapy (CBT), motivational enhancement, and contingency management. There is no FDA-approved medication for cannabis use disorder. Treatment works through behavioural change — identifying triggers, restructuring thoughts around use, and rebuilding the daily routine that cannabis was filling.
NIDA’s reviews of cannabis treatment consistently identify CBT, motivational enhancement therapy, and contingency management as the most effective approaches (NIDA, 2024). At One Step we run a CBT-based programme alongside DBT components for emotional regulation — the irritability and mood volatility of cannabis withdrawal respond well to DBT distress tolerance skills.
A few specifics on what we work on with cannabis-dependent clients:
- Trigger mapping. Cannabis use is heavily cue-driven — particular times of day, particular friends, particular activities. Identifying these in writing during week one is the foundation.
- Behavioural substitution. Cannabis fills time. Working out what you actually do at 9pm now that you’re not getting high is the bigger question than how to resist a craving.
- Sleep restoration. Sleep hygiene is treated as a clinical intervention, not an afterthought.
- Cue exposure. Especially in week three and beyond, controlled exposure to triggers without using is how cravings extinguish.

How Does One Step Handle Cannabis Discontinuation?
One Step provides supportive on-site management for cannabis discontinuation as part of our standard residential programme. Cannabis withdrawal doesn’t require medical detox because no medication is needed for the body to safely come off it — but the peak (days 3-7) is much easier to get through in a structured residential setting with no access to cannabis, no triggers from your usual environment, and people around you who understand what you’re going through.
What this looks like in practice at our residential programme in Chiang Mai:
- Intake and assessment. Our visiting psychiatrist reviews your use history on arrival. If you’ve also been using other substances regularly — alcohol, benzodiazepines, opioids — we screen for whether you need a different approach first.
- Structured days from day one. Our daily schedule starts at 7am with morning meditation. Group therapy 9-11. Activities in the afternoon. This structure is the single biggest reason cannabis discontinuation is easier in residential than at home.
- Sleep support through the peak. We work with you on sleep hygiene from day one. Where appropriate, our visiting psychiatrist can prescribe short-term non-addictive medication for sleep through the worst nights — billed separately, as with all prescribed medication.
- Daily aerobic exercise and outdoor time. Our excursion programme gets you out of the facility regularly — temple visits, hikes, walks. Daylight and movement are real interventions for the sleep and mood disruption of cannabis withdrawal.
- CBT-based therapy. Individual and group sessions focus on trigger mapping, behavioural substitution, and relapse planning.
The programme costs roughly ฿280,000/month (~$8,500 USD). That covers your accommodation, food, therapy, activities, and intake assessment with our visiting psychiatrist. Medication prescribed during your stay — including any sleep aids — is billed separately. Flights, visas, and personal items are not included. The full breakdown is on our pricing page.
Most cannabis clients stay 28-60 days. Shorter than 28 and you’ve barely cleared the acute window. Longer than 60 is uncommon for cannabis-only cases, though we have it available for clients with co-occurring conditions like depression or anxiety disorders that need longer therapeutic work. We also run a cannabis-specific track within the wider rehab programme for clients whose primary issue is heavy long-term cannabis use.
When Does Residential Cannabis Rehab Actually Make Sense?
Residential rehab for cannabis makes sense when you’ve tried to quit on your own and got stuck at the peak, when your home environment has too many triggers (housemates who use, social network built around cannabis), when daily heavy use has been going on for years, when sleep collapse during withdrawal has been the specific reason for past relapses, or when there’s an underlying anxiety or depression that’s been masked by daily use.
Plenty of cannabis users can stop without residential treatment. If your use has been recent or moderate, your home environment is stable, and you have accountability in place, outpatient support and CBT may be enough. Residential becomes the right call when the structural problems outweigh the willpower problem — and they usually do for heavy long-term users.
Frequently Asked Questions
Common questions about cannabis withdrawal symptoms and timeline.
Acute cannabis withdrawal symptoms typically start within 24-48 hours, peak between days 3 and 7, and resolve over 2-3 weeks for most people. Heavy long-term users may experience intermittent post-acute symptoms — particularly sleep disturbance and cue-triggered cravings — for several weeks to a few months after stopping.
No. Unlike alcohol or benzodiazepine withdrawal, cannabis withdrawal is not life-threatening — there is no seizure or delirium risk. It is genuinely uncomfortable and the peak can feel overwhelming, but the body comes off cannabis safely without medical detox. The biggest practical risk is substituting alcohol or other substances to cope, which is more dangerous than the withdrawal itself.
Cannabis suppresses REM sleep with daily use. When you stop, your brain rebounds with extra REM, vivid dreams, and disrupted sleep architecture — taking longer to fall asleep, waking more often, and getting less deep sleep. Sleep is typically the last withdrawal symptom to fully resolve, often taking several weeks. Consistent sleep hygiene helps, and short-term non-addictive sleep support can be appropriate for the peak.
Not always. Many cannabis users can stop with outpatient support, accountability, and CBT. Residential rehab makes sense when previous attempts have failed at the peak, when your home environment is full of triggers, when use has been daily and heavy for years, or when there are co-occurring mental health conditions that have been masked by daily cannabis use.
A 2020 meta-analysis pooling data from over 23,500 cannabis users found roughly 47% experience meaningful withdrawal symptoms when they stop. The rate climbs to 54% in outpatient clinical settings and 87% in inpatient settings. Daily users, those who also use tobacco, and those with cannabis use disorder are far more likely to experience full withdrawal.
There is no FDA-approved medication specifically for cannabis withdrawal or cannabis use disorder. Treatment is primarily behavioural — CBT, motivational enhancement, contingency management. Short-term symptomatic support (such as non-addictive sleep medication for the peak) may be prescribed but is not the foundation of treatment.
For most people, days 3 through 7 are the hardest. Sleep is at its worst, sweating and restlessness peak, cravings spike, and appetite is gone. Day 4 or 5 is when most unaided quit attempts fail. If you can get past day 7 without using, the trajectory clearly improves from there.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn