Key Takeaways
- Residential treatment resets the nervous system and builds skills, but the brain takes 12–18 months to rewire after heavy meth use — most of that work happens after discharge.
- The first 90 days post-treatment are the highest-risk window. Roughly 61% of people relapse within a year of leaving treatment if aftercare is weak or absent.
- Meth aftercare differs from alcohol or opioid aftercare: no FDA-approved anti-craving medication, longer joyless period (anhedonia), and sleep that takes 6+ months to normalise.
- Real aftercare is structured and scheduled — weekly therapy, a peer group (CMA, NA, or SMART Recovery), sober community, sleep monitoring, and family integration — not “just go to two meetings a week.”
- Aftercare only works if the client shows up. Programmes can structure it, accountability tools can support it, but the daily decision is the client’s.
Meth recovery is not a 30-day fix. Residential treatment resets your nervous system, breaks the using pattern, and gives you the skills — but the brain takes 12 to 18 months to rewire after heavy methamphetamine use, and relapse curves stay steep until you cross the one-year mark. Roughly 61% of people relapse within 12 months of leaving treatment, with the first 90 days the highest-risk window (Brecht & Herbeck, Drug Alcohol Depend, 2014). Aftercare is where the actual recovery happens. This guide explains what good meth aftercare looks like, why it matters more for meth than for most other substances, and what One Step provides after you finish the residential meth rehab programme.
Why Is Residential Treatment Only the Start of Meth Recovery?
Residential treatment does three things well: it removes the drug, resets your sleep and appetite, and teaches you the skills to handle cravings. What it cannot do is give you a year of clean cue exposure, walk you through the first real-world crisis, or weather the months when your brain still hasn’t restored normal pleasure response. That work has to happen outside the unit.
PET imaging shows that dopamine transporter levels in heavy meth users only approach normal after 12 to 17 months of abstinence (Volkow et al., J Neurosci, 2001). Until then, motivation is blunted, ordinary pleasures feel flat, and stress sets cravings off easily. A 30 to 60-day residential stay gets you through the worst withdrawal and lays the groundwork — but it ends long before the brain has finished its repair work.
The other thing residential treatment can’t do is expose you to the real cues that will trigger you: the friend who used to use with you, the bedroom where you stayed up for three days, the payday, the bad argument with a partner. You only meet those cues sober for the first time after you leave. Without structured aftercare, that first encounter often becomes the first relapse.

How Long Is the High-Risk Window After Meth Treatment?
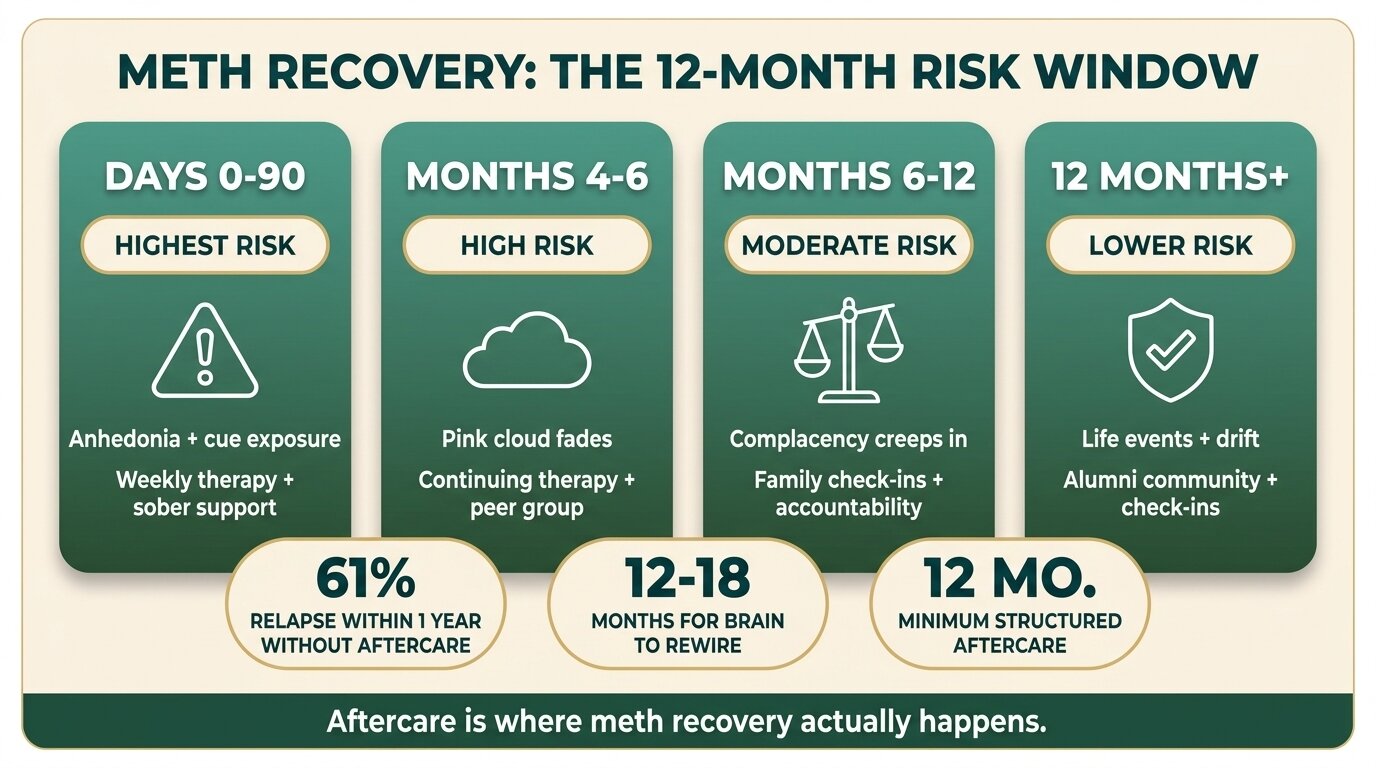
The first 90 days after leaving treatment carry the highest relapse risk, followed by months four to six, and then six to twelve. Relapse curves bend after the one-year mark but do not flatten — meth use disorder is a chronic, relapsing condition that needs ongoing support, not a problem you solve once and walk away from.
A long-term study tracking people after treatment for methamphetamine use found that 61% relapsed within the first year of discharge, with a further 14% relapsing in years two through five (Brecht & Herbeck, Drug Alcohol Depend, 2014). The same study identified longer treatment duration and participation in self-help or additional treatment after discharge as the strongest protective factors. In plain terms: people who stayed engaged with care after they left did much better than people who didn’t.
| Window | Risk level | What’s driving it | What helps most |
|---|---|---|---|
| Days 0–90 | Highest | Anhedonia, sleep disruption, cue exposure, low motivation | Daily structure, weekly therapy, sober living or close family supervision |
| Months 4–6 | High | “Pink cloud” fading, return to old environment, first stressors | Continuing therapy, peer group attendance, sponsor or peer mentor |
| Months 6–12 | Moderate | Complacency, perceived recovery, occasional cravings | Family check-ins, accountability tools, ongoing peer connection |
| 12 months+ | Lower but never zero | Major life events, unprocessed trauma, polysubstance drift | Alumni community, lifelong meeting habit, scheduled check-ins |
Why Is Meth Aftercare Different From Alcohol or Opioid Aftercare?
Meth aftercare is harder because there is no FDA-approved anti-craving medication, the joyless period after stopping lasts longer than with most substances, sleep stays wrecked for six months or more, and cravings remain strong well into the first year. You can’t lean on naltrexone, buprenorphine, or acamprosate to take the edge off — the structure has to do all the work.
For alcohol use disorder, naltrexone or acamprosate can blunt cravings. For opioid use disorder, buprenorphine or methadone can occupy receptors and remove the daily craving entirely. For methamphetamine, no medication has the same effect. NIDA-funded research has identified some promising combinations (such as bupropion plus injectable naltrexone), but no single approved medication exists that prevents meth cravings the way agonist therapy works for opioids (NIDA, 2024).
The result: meth aftercare leans much harder on behavioural structure than on pharmacology. Contingency management — small, tangible incentives for negative drug tests — has the strongest evidence base of any psychosocial intervention for stimulant use disorder, but it is rarely available outside research settings or specific U.S. clinics (SAMHSA TIP 33, 2021). For most people in international recovery, the aftercare stack is therapy plus peer group plus sober community plus sleep work — and consistency over many months is what makes it work.
The sleep problem specifically
Heavy meth use destroys sleep architecture. Many people leave residential treatment still sleeping badly — falling asleep is hard, staying asleep is harder, and REM rebound dreams are vivid and disturbing. Sleep typically takes six months or more to normalise. Poor sleep is itself a relapse trigger because exhaustion blunts judgment and intensifies cravings. If you’ve struggled with sleep without alcohol, the parallels apply here — see our guide on how to fix broken sleep in recovery.

What Does Good Meth Aftercare Actually Look Like?
Good meth aftercare is structured, scheduled, and accountable. It combines weekly individual therapy, a peer support group, sober community for the early phase, medication management for any co-occurring conditions, sleep monitoring, family or partner integration, and where available, contingency management or random urine testing as a client-requested accountability tool. “Go to NA twice a week” is not aftercare — it’s the absence of a plan.
Continuing care research consistently shows that interventions producing longer planned treatment duration and using active outreach to the client tend to yield better outcomes (McKay, J Subst Abuse Treat, 2009). The mechanism is simple: people who relapse don’t usually call their counsellor — but if the counsellor calls them, they re-engage. Active outreach beats passive availability.
The components of a real meth aftercare plan
- Weekly individual therapy — CBT for craving management, dual-diagnosis follow-up if depression, ADHD, anxiety, or trauma is part of the picture. Read more about how CBT and DBT support addiction recovery.
- A peer support group — Crystal Meth Anonymous (CMA), Narcotics Anonymous (NA), or SMART Recovery. Pick one and commit. Two to four meetings a week is typical for the first year.
- Sober community or sober living for the early phase, especially if your home environment includes people who still use or places strongly associated with using.
- Medication management for any co-occurring depression, ADHD, anxiety, or sleep issue. Stimulant use often masks underlying conditions that resurface once you stop using.
- Sleep monitoring for the first six months. Track hours, quality, dream content. Poor sleep is an early warning sign, not just a side effect.
- Family or partner integration so cravings get spoken, not hidden. Hidden cravings turn into relapses. A partner who can ask “how’s it sitting today?” and get an honest answer is one of the strongest protective factors.
- Random urine testing if the client requests it as an accountability tool. Many people in early recovery ask for testing because the prospect of a positive test gives them a concrete reason to say no in the moment.
- Contingency management where available — small incentives for negative tests have the strongest evidence base for stimulant use disorder.
The first time I see a client relapse after a strong residential stay, it’s almost never because the programme failed. It’s because the aftercare plan said “go to NA” and that was it. Real meth aftercare is a weekly therapy slot, a peer group, a sober roommate or family member, and someone who notices when you go quiet. Without that structure, the brain’s still healing and the cues are still loaded — relapse is just a matter of which Tuesday it happens on.
Craig GagnonSenior Therapist, One Step Rehab
Worried that your aftercare plan won’t hold? Talk to our team — we’ll walk you through what a realistic post-discharge structure looks like for your situation.
What Is “The Aftercare Gap” and Why Do So Many People Fall Through It?
The aftercare gap is the space between what a programme discharges you with and what actual continuing care looks like. Many facilities hand clients a paper plan that says “attend two NA meetings a week and follow up with your GP” and call it aftercare. That’s not aftercare — that’s a goodbye letter. Real continuing care is scheduled, accountable, and involves active outreach when contact lapses.
This gap exists for two reasons. One, aftercare is unbillable in many systems — facilities are paid for the residential stay, not the year that follows. Two, clients leave residential treatment feeling much better than when they arrived, which gives both the client and the discharge planner false confidence. Three weeks of clean sleep and structured days creates a fragile pink cloud that masks how much support the brain still needs.
The Brecht and Herbeck data is the clearest signal here: 61% relapse within a year if aftercare is weak or absent, and the protective factor that stood out across the analysis was post-discharge participation in continuing care or self-help (Brecht & Herbeck, Drug Alcohol Depend, 2014). If your discharge plan reads like a checklist someone could complete in 20 minutes, it’s not enough.

What Aftercare Does One Step Rehab Provide?
One Step provides weekly aftercare calls, an alumni community, Zoom group support, and family coaching for clients who finish the residential programme. The aftercare is included in the residential fee — not billed separately — and runs for the first 12 months after discharge. It is intentionally structured around the real high-risk windows: weekly contact for the first 90 days, then tapering frequency through months four to twelve.
What that looks like in practice:
- Weekly one-to-one aftercare call with your assigned counsellor for the first 12 weeks, then fortnightly through month six, then monthly through month twelve. Call format is flexible — voice, video, or messaging — but the slot is scheduled and the counsellor initiates if you don’t.
- Zoom group support meeting open to all alumni — a weekly facilitated check-in where current and recent alumni share craving patterns, wins, and slips. Most people find one group call a week useful for the first six months.
- Alumni WhatsApp community for between-call support — useful for the 3 a.m. craving and the random Tuesday when you need to talk to someone who gets it.
- Family coaching sessions through the family programme — so the people around you know what to look for, how to ask, and when to step back. Hidden cravings are the most common precursor to a meth relapse; a family that can hold the conversation makes hidden cravings rare.
- Re-entry support if you slip — a relapse doesn’t end the relationship. We help you assess whether a brief return for residential top-up makes sense, or whether outpatient intensification (more frequent calls, a peer reconnect) is enough.
The residential programme costs about ฿280,000/month (~$8,500 USD), and the 12 months of aftercare are part of that fee. Medication prescribed during your stay, flights, visa, hospital visits, and personal items are billed separately — see the pricing page for the full exclusion list.
What we don’t do
We don’t run a U.S.-style contingency management programme with cash incentives for negative tests — that infrastructure isn’t available where we operate. We don’t provide sober living after discharge — we can refer to options in Chiang Mai, Bangkok, or your home country, but we are a residential programme, not a halfway house. We don’t replace local treatment relationships — if you have a psychiatrist or therapist at home, our aftercare augments theirs, it doesn’t substitute.

What Does the Client Have to Do for Aftercare to Work?
Aftercare is a partnership, not a service the client receives passively. The programme can structure it, the counsellor can call, the family can show up — but the client has to answer the call, attend the meeting, be honest about cravings, and treat the first year as the priority it actually is. Most people who succeed treat year one like a full-time job.
The specific behaviours that separate people who stay clean from people who don’t, in our experience running the programme:
- Answering the aftercare call on the day it’s scheduled. When clients start ducking calls, relapse is usually already in motion.
- Naming cravings out loud the day they happen — to the counsellor, the sponsor, the partner, the meeting. Cravings that get spoken lose most of their power. Cravings that get hidden grow.
- Going to the meeting even when you don’t feel like it. Especially when you don’t feel like it. The drop in motivation is itself part of the meth brain’s recovery curve — it lifts, but only if you keep showing up while it’s still flat.
- Avoiding the obvious cues for the first year. The friend who used to use, the bar where you bought, the dating app where you scored. You can rebuild those relationships later or replace them entirely — not in month three.
- Treating sleep, food, and exercise as non-negotiable. Sleep deprivation is a craving multiplier. Skipping meals drops blood sugar and mood. Sitting at home all day grows the boredom that meth used to fill.
For more on what to plan around in the early months, see our guide to the 10 most common relapse triggers and how to plan for each, and our piece on reducing relapse risk during the withdrawal window.
If you or someone you love is struggling with substance dependence, explore how a comprehensive drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions About Meth Aftercare
Common questions about what aftercare looks like after meth rehab and how long it should last.
At minimum 12 months of structured contact, because the brain takes 12 to 18 months to rewire after heavy meth use and relapse curves stay steep until you cross the one-year mark. Many people benefit from continued peer-group attendance and periodic check-ins for longer.
No medication is approved specifically to prevent methamphetamine cravings the way naltrexone works for alcohol or buprenorphine for opioids. Research on combinations like bupropion plus injectable naltrexone is promising, but for now meth aftercare leans on behavioural structure rather than pharmacology.
Crystal Meth Anonymous (CMA) is a 12-step group specifically for methamphetamine recovery. Narcotics Anonymous (NA) is a 12-step group for any drug. SMART Recovery is a secular, CBT-based programme without sponsorship. All three work — the best one is the one you’ll actually attend regularly.
If your home environment includes people who still use, places strongly tied to your using, or no sober support, sober living for the first three to six months substantially lowers relapse risk. If you have a supportive partner or family and a stable home, structured outpatient aftercare may be enough.
A relapse does not end your relationship with the programme. The honest first move is telling your counsellor or sponsor that day. At One Step we then assess whether a brief return for residential top-up makes sense or whether intensifying outpatient contact is enough. Hidden relapses are the dangerous ones — spoken ones are recoverable.
Yes. Twelve months of structured aftercare — weekly calls tapering to monthly, Zoom group meetings, alumni community access, and family coaching — are included in the residential programme fee. Medication, flights, visas, and personal items remain billed separately.
Meth aftercare runs longer, leans harder on behavioural structure, and includes specific attention to sleep recovery because meth wrecks sleep architecture for six months or more. Alcohol aftercare can use anti-craving medication; meth aftercare cannot. The joyless period after stopping is typically longer for meth than for alcohol or opioids.
Written by
Craig Gagnon
Craig Cagnon is an American counseling psychologist and addiction counselor. He holds Masters degrees in community counseling and counseling psychology and completed his clinical residency at The Mayo Clinic, in Rochest...
Learn more about Craig
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn