
Key Takeaways
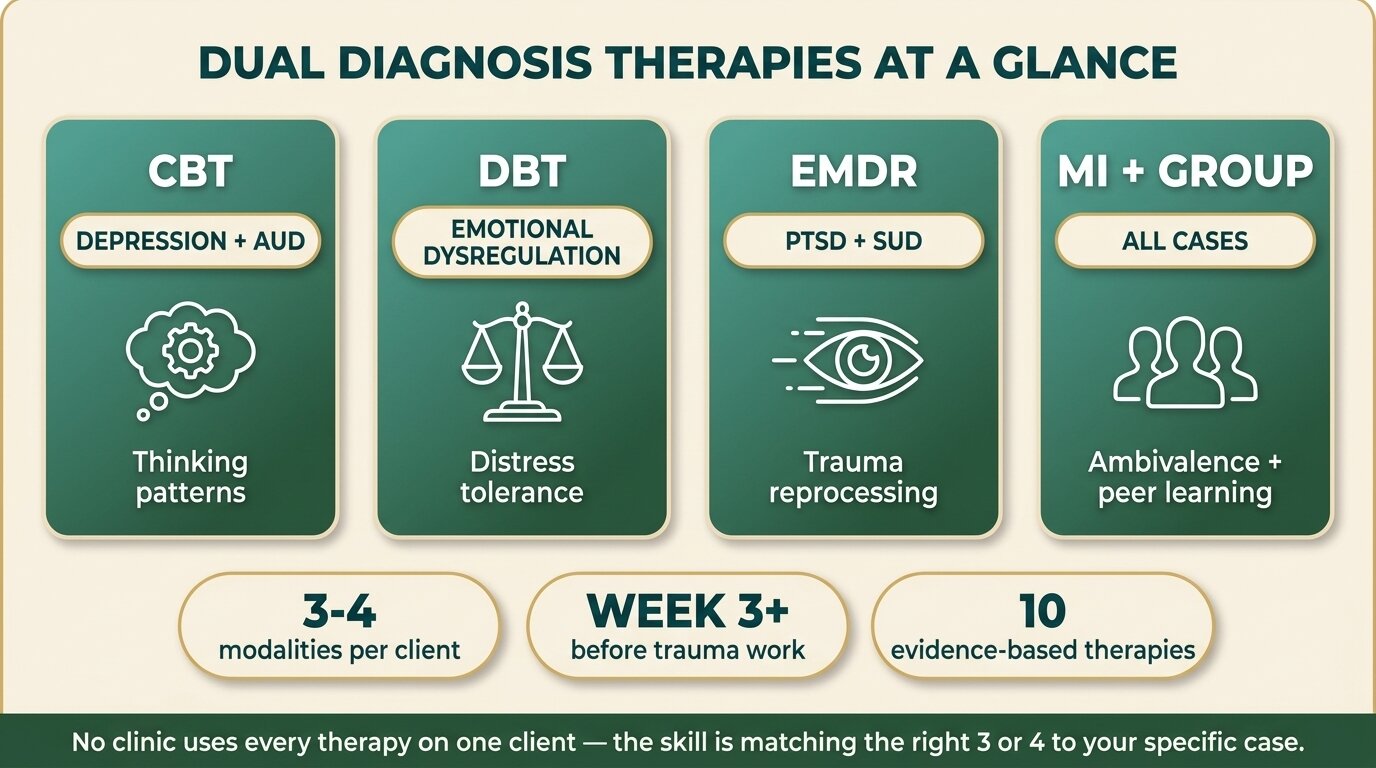
- There are roughly ten distinct therapies used in dual diagnosis treatment. No clinic uses all of them on one client — the work is in matching the right three or four to the specific combination of substance use disorder and psychiatric diagnosis.
- CBT and DBT are the spine for most cases. CBT targets distorted thinking patterns (depression, anxiety). DBT targets emotional dysregulation (borderline traits, self-harm history, suicidality). Most clients use elements of both.
- EMDR and trauma-focused CBT (TF-CBT) are reserved for trauma-driven addiction — PTSD with opioid, alcohol, or benzodiazepine use. They do not start in week one. The client has to be stable, sober, and sleeping first.
- Motivational interviewing (MI) runs through every other modality; ACT is useful for chronic depression and values-based recovery; schema therapy is a long-term modality for personality patterns underneath both conditions.
- At One Step, the working mix is CBT, DBT, EMDR for trauma, MI throughout, group therapy, and family work — with psychiatric medication managed by our visiting consultant psychiatrist. We do not offer schema therapy as a primary modality; for that we would refer.
The therapies used in dual diagnosis treatment are not interchangeable — each one solves a different clinical problem. CBT changes thoughts. DBT regulates emotions. EMDR processes trauma. Motivational interviewing handles ambivalence. ACT works on values when depression is chronic. Schema therapy unpicks lifelong patterns. The skill of dual diagnosis treatment is matching three or four of these to the specific combination of substance and psychiatric diagnosis the client arrived with — and dropping the rest. Integrated treatment using a combination of evidence-based psychotherapies is the current standard of care (SAMHSA TIP 42, 2020).
How Does CBT Work for Dual Diagnosis?
Cognitive Behavioural Therapy (CBT) treats dual diagnosis by changing the thought-behaviour loop that drives both conditions. For depression plus alcohol use disorder, that means catching the catastrophic thinking that triggers drinking. For anxiety plus stimulant use, it means breaking the avoidance pattern that keeps anxiety alive. CBT is the first-line therapy for most mood and anxiety combinations with substance use.
CBT is structured, time-limited, and skills-based. The therapist and client identify the thinking patterns — “I cannot cope with this without a drink”, “if I do not use I will not be able to function at work”, “everyone can see I am anxious” — and test them against the evidence. Behavioural experiments follow: the client deliberately enters a feared situation without using and records what actually happens.
A 2014 meta-analysis of twelve trials with 1,721 patients found that CBT combined with motivational interviewing produced significant improvements in both alcohol consumption and depressive symptoms compared with controls (Riper et al., Addiction, 2014). The effect sizes are modest, not miraculous — CBT works, but it is one piece of an integrated plan rather than a standalone fix.
What CBT is good at: mood and anxiety disorders co-occurring with substance use, identifying and changing high-risk thinking, relapse prevention, sleep restoration. What it is less suited to: severe trauma (use EMDR or TF-CBT instead), entrenched personality patterns (schema therapy fits better), emotional dysregulation severe enough that the client cannot use the thinking skills (DBT comes first). Our breakdown of CBT vs DBT for addiction covers the practical differences in detail.

When Is DBT the Right Therapy Instead of CBT?
Dialectical Behaviour Therapy (DBT) is the right choice when the underlying problem is emotional dysregulation rather than distorted thinking. It is first-line for borderline personality traits, a history of self-harm, suicidality, or chronic emotional crises that co-occur with substance use. DBT teaches concrete skills — distress tolerance, emotion regulation, mindfulness, interpersonal effectiveness — that work when feelings escalate too fast for CBT-style cognitive work to land.
The clearest evidence for DBT in dual diagnosis comes from Marsha Linehan’s foundational randomised trial in drug-dependent women with borderline personality disorder. DBT produced significantly greater reductions in drug use, measured both by structured interview and urinalysis, compared with treatment as usual (Linehan et al., Am J Addict, 1999). Since then DBT for Substance Use Disorders has been adapted and tested across multiple populations with consistent results.
DBT has four core skill modules. Distress tolerance teaches the client to get through a crisis without making it worse — useful when the previous crisis-management tool was a substance. Emotion regulation teaches the client to identify, label, and shift emotional intensity. Mindfulness builds the capacity to observe an urge without acting on it. Interpersonal effectiveness teaches how to set limits and ask for what is needed without escalating into conflict.
For dual diagnosis specifically, DBT shines in cases where CBT keeps stalling. A client who intellectually understands the cognitive distortions but still gets hijacked by emotional intensity is a DBT candidate, not a CBT candidate. Most residential dual diagnosis clients get a mix — DBT skills training in the early weeks to stabilise emotional reactivity, CBT in the middle weeks to work on thinking patterns once the client can tolerate the work.

When Should EMDR Be Used for Dual Diagnosis?
Eye Movement Desensitisation and Reprocessing (EMDR) should be used when the addiction is trauma-driven — when PTSD, complex trauma, or significant adverse childhood experiences sit underneath the substance use. EMDR is first-line for PTSD co-occurring with opioid, alcohol, or benzodiazepine use. It is not used in week one; the client needs to be stable, sober, and sleeping before trauma reprocessing begins.
EMDR uses bilateral stimulation — typically guided eye movements — while the client briefly holds a target memory in mind. The mechanism is debated; the outcomes are not. A 2025 randomised controlled trial comparing prolonged exposure, EMDR, and imagery rescripting against substance use disorder treatment alone found that EMDR added to SUD treatment produced a mean reduction of nearly 8 points on the CAPS-5 PTSD severity scale compared with SUD treatment alone, without worsening substance use outcomes (Lortye et al., Addiction, 2025).
The sequencing rule is non-negotiable. Starting trauma reprocessing in early withdrawal makes symptoms worse. The client needs roughly two to four weeks of stabilisation work — grounding skills, daily structure, sleep restoration, sometimes medication adjustment — before EMDR can begin. Skipping this phase is one of the classic mistakes in dual diagnosis treatment.
EMDR is delivered by a specifically trained therapist in individual sessions, not group settings. Most clients need eight to twelve sessions for a single trauma target; complex trauma with multiple targets takes longer. For residential treatment of 60 to 90 days, that means EMDR work usually runs from week three or four through to discharge, with the trauma processing carefully paced against the rest of the recovery work.
How Is Trauma-Focused CBT Different from Regular CBT?
Trauma-Focused CBT (TF-CBT) is a distinct structured protocol for trauma processing, not just “CBT with trauma themes”. It combines cognitive-behavioural skills with structured exposure to the trauma narrative, gradual cognitive processing of trauma-related beliefs, and stabilisation work. TF-CBT and EMDR are the two trauma modalities with the strongest evidence base for PTSD; clinical preference and client tolerance decide which is used.
Where regular CBT might address trauma-related thoughts as one element among many, TF-CBT puts the trauma narrative at the centre. The client gradually writes or speaks the trauma story across sessions, building tolerance for the material, while the therapist helps reframe the meaning attached to it. Originally developed for children and adolescents, the protocol has been adapted for adults and consistently shows large effects on PTSD symptoms.
For dual diagnosis, TF-CBT is most often used when the trauma is recent and well-defined — a specific assault, an accident, a combat exposure — rather than diffuse complex trauma running from childhood. EMDR tends to be the choice for the latter. Some clinicians prefer TF-CBT because the structure is fully cognitive and verbal, which suits clients who find the bilateral stimulation component of EMDR uncomfortable.
What Does Motivational Interviewing Do in Dual Diagnosis Treatment?
Motivational Interviewing (MI) does the work of moving a client from ambivalence into action. It is not a standalone treatment for dual diagnosis; it is the conversational style that runs through every other modality. MI is the right tool when a client is intellectually aware of the problem but emotionally stuck — half wanting to change, half not — which describes most people entering dual diagnosis treatment.
MI is built on four processes: engaging the client, focusing on what needs to change, evoking the client’s own reasons for change, and planning. The therapist does not argue, lecture, or persuade — they elicit. The technique looks deceptively simple. The skill is in reflecting what the client says, amplifying the change-talk that emerges, and steering away from the resistance-talk that drives people deeper into ambivalence.
A meta-analysis of 119 studies found MI produced significant durable effects on substance use outcomes when compared with weak control conditions, with effect sizes in the small-to-moderate range; against specific active treatments, MI was roughly equivalent rather than superior (Lundahl et al., Res Soc Work Pract, 2010). The practical takeaway: MI works as a way of conducting therapy, not as the therapy itself.
In dual diagnosis, MI is particularly useful in the first two weeks when the client is still negotiating with themselves about whether to commit to the work, and at decision points later in treatment — whether to start an antidepressant, whether to engage in trauma work, whether to involve family. A skilled MI therapist makes those moments productive rather than confrontational.
When Is ACT the Right Therapy for Dual Diagnosis?
Acceptance and Commitment Therapy (ACT) is the right choice when depression is chronic, when the client has been through multiple rounds of treatment, or when the recovery work needs to be values-based rather than symptom-focused. ACT does not try to eliminate uncomfortable thoughts and feelings; it teaches the client to act in line with their values regardless of what their mind is doing. That makes it well-suited to long-term recovery, where some level of discomfort is permanent.
The ACT framework rests on six processes: acceptance of difficult internal experiences, cognitive defusion (seeing thoughts as thoughts, not facts), present-moment awareness, self-as-context, values clarification, and committed action. For dual diagnosis, the values piece is often the lever. A client who has lost touch with what they actually care about — beyond not using — has nothing to recover towards. ACT makes the recovery direction explicit.
An initial meta-analysis of ten randomised trials with 1,386 participants found a small-to-medium effect size favouring ACT over active treatment comparisons for substance use outcomes (Lee et al., Drug Alcohol Depend, 2015). The evidence base is smaller than CBT’s but consistent. ACT is now a recognised evidence-based option, particularly for chronic and relapsing presentations.
Does Dual Diagnosis Need Schema Therapy?
Schema therapy is needed when long-standing personality patterns — perfectionism, abandonment fears, emotional deprivation, mistrust — underlie both the substance use and the psychiatric condition. It is a longer-term modality, typically delivered over a year or more, that targets the early-formed schemas driving repeated relapse and chronic dysfunction. Schema therapy is most often used for borderline personality disorder, complex trauma, and treatment-resistant cases.
The flagship trial by Giesen-Bloo and colleagues compared schema therapy with transference-focused psychotherapy for borderline personality disorder over three years and found schema therapy more effective on most outcomes, with large effect sizes for both treatments (Giesen-Bloo et al., Arch Gen Psychiatry, 2006). Subsequent meta-analyses have replicated the finding that schema therapy produces durable change in personality patterns.
The honest limitation: schema therapy is a long modality that does not fit easily into a 60-to-90-day residential stay. Most residential programmes — including ours — use schema-informed elements within DBT and individual therapy rather than running a full schema therapy protocol. If schema therapy is the indicated treatment, the right plan is residential rehab for stabilisation and substance use work, then long-term schema therapy with a specialist outpatient clinician afterwards.
People come into treatment expecting one therapy to fix it. The reality is that we are choosing three or four modalities from a menu, in a specific sequence, for a specific case. CBT in the first month is rarely the same person’s CBT in the second month — by then we are usually doing DBT skills work, or starting EMDR if the trauma is what is driving the using. The art is in the sequencing and the matching. Get that wrong and the best therapy in the world will not stick.
Alastair MordeyProgramme Director, One Step Rehab
How Does Group Therapy Fit Into Dual Diagnosis?
Group therapy in dual diagnosis serves three jobs that individual therapy cannot do: peer learning from people facing similar combinations, accountability that comes from being known by others in treatment, and normalising the dual diagnosis experience so the client stops feeling uniquely broken. Process groups, relapse prevention groups, and skills-training groups are the standard formats. Group work runs alongside individual therapy, not instead of it.
A systematic review and meta-analysis of group treatment for substance use disorders found significant small-to-moderate effects on abstinence compared with no treatment and with individual therapy alone (Lo Coco et al., J Subst Abuse Treat, 2019). The mental-health benefits of group work are similar. The mechanism is partly therapeutic content, partly the social structure of being in a room with others doing the same work.
For dual diagnosis, the group composition matters. A client with depression and alcohol use disorder in a substance-only group can feel like the only person whose head is the real problem; the same client in a group where others are working on mood disorders and trauma normalises the work. The trade-off: a smaller pool of clients with overlapping presentations may mean less group time on substance-specific content. Most residential dual diagnosis programmes — ours included — run mixed-presentation groups for that reason.
Not sure which therapies your situation actually needs? Talk to our team — we will be specific about which modalities apply to your case and which do not.

When Is Family Therapy Part of the Dual Diagnosis Plan?
Family therapy is part of the dual diagnosis plan when the family system maintains either condition — when family dynamics drive the drinking, when an unwell relationship with a partner sustains the depression, or when family will be the primary support structure in aftercare. Behavioural couples therapy and family systems work both have meta-analytic support showing better substance use outcomes and better relationship functioning compared with individual treatment alone.
The decision point is whether the family is part of the problem, part of the solution, or both. A spouse who controls and enables in equal measure shows up in both columns. A parent who has been managing the addiction for a decade carries trauma of their own that needs to be heard. The family piece can be the difference between a clean discharge and a relapse within two weeks of getting home.
Practically, family work in residential treatment looks like structured video calls, dedicated family weekend sessions, and a planned re-entry conversation before discharge. Where geography allows, in-person family sessions later in the stay are more productive than early ones — the client needs to be stable enough to participate without escalating. Our family programme covers how this is structured day to day.
Where Does Psychiatric Medication Fit in the Therapy Mix?
Psychiatric medication is not a therapy, but it is part of the integrated treatment plan in most dual diagnosis cases. Antidepressants, mood stabilisers, anti-craving medications, and sleep medications work alongside the psychological therapies — neither replaces the other. NICE guideline NG58 and SAMHSA TIP 42 both treat medication management and psychological therapy as parallel components of integrated treatment (NICE NG58, 2016).
For depression with alcohol use disorder, an SSRI is usually started after detox stabilises. For PTSD, an SSRI or SNRI is standard, with prazosin sometimes added for trauma-related nightmares. For alcohol use disorder, naltrexone or acamprosate may be added to reduce craving. For bipolar plus substance use, mood-stabilising medication is essential — the therapy work cannot land if mood is swinging through clinical extremes.
Medication decisions are made by a psychiatrist, not by the therapy team. At residential level, this typically means a visiting consultant psychiatrist who assesses on intake, prescribes or adjusts during the stay, and hands over to the client’s home psychiatrist at discharge. The medication itself is billed separately from the programme fee — the same way medication outside rehab is paid for.
Which Therapy Goes with Which Dual Diagnosis Combination?
Matching the right therapy to the specific dual diagnosis is the central skill of integrated treatment. There is no universal “dual diagnosis programme” — different combinations of substance and psychiatric diagnosis call for different first-line modalities. The table below summarises the matches that the dual diagnosis evidence base most consistently supports.
| Combination | First-line therapy | Common additions |
|---|---|---|
| Depression + alcohol use disorder | CBT + behavioural activation | MI throughout, group therapy, SSRI |
| Anxiety + stimulant use (cocaine, meth) | CBT for anxiety + exposure work | MI, mindfulness skills, sleep work |
| PTSD + opioid / alcohol / benzo use | Stabilisation first, then EMDR or TF-CBT | SSRI, grounding skills, group work |
| Borderline traits + substance use | DBT (full skills training) | Schema-informed work, family therapy |
| Bipolar II (stable) + substance use | Psychoeducation + DBT skills | Mood stabiliser, sleep and routine work |
| ADHD + substance use | Structure-heavy CBT | Behavioural skills, cautious medication review |
| Chronic depression + long-term recovery | ACT (values-based work) | CBT, schema-informed elements |
| Complex trauma + treatment-resistant addiction | Schema therapy (long-term outpatient) | Residential stabilisation first, then ongoing schema work |
Two things this table does not capture. First, the matches are starting points — clinical observation in the first two weeks often shifts the plan. Second, every line item assumes the client is medically stable and has completed any necessary detox; trauma work and personality work cannot start in withdrawal.
Which Therapies Does One Step Actually Use?
At One Step the working therapy mix is CBT, DBT, EMDR for trauma cases, motivational interviewing running through everything, group therapy, and family work. Psychiatric medication is managed by our visiting consultant psychiatrist. We do not run schema therapy as a primary modality — when a case calls for full schema work we use schema-informed elements within DBT, then refer to a specialist clinician for the long-term schema therapy after discharge.
The spine for most clients is CBT plus DBT skills training. The proportion shifts by diagnosis: depression-led cases lean CBT-heavy, emotionally dysregulated cases lean DBT-heavy. EMDR is added for clients with confirmed PTSD or significant trauma history, starting no earlier than week three once stabilisation work has done its job. Motivational interviewing is woven through individual sessions from day one — the therapeutic style, not a separate slot.
Group therapy runs throughout the stay across all clients — process group, relapse prevention, skills training. Family work is offered to every client and engaged where the family is part of the picture. The treatment schedule shows how individual and group sessions sit alongside each other in the daily structure.
For broader context on how we approach co-occurring conditions across the programme, our dual diagnosis treatment page covers the clinical structure, and our companion post on personalised dual diagnosis therapy covers how a plan is actually built case by case. For the underlying decision about whether residential treatment is the right setting at all, our inpatient vs outpatient comparison covers the trade-offs.
One Step is a residential treatment centre in Chiang Mai running structured programmes of 28 days and longer. The fee is approximately ฿280,000/month (around $8,500 USD). What is included in the fee: accommodation, meals, group therapy, individual therapy sessions, group activities, intake psychiatric assessment and routine progress checks with our visiting psychiatrist. What is not included: medication prescribed during the stay, flights, visas, supplements, additional counselling sessions beyond the programme allocation, hospital visits, and personal items. The pricing page lists the exclusions in full.
Two honest limits on what residential dual diagnosis at One Step can do. First, we are not a locked psychiatric facility — active psychosis, acute suicidal crisis with intent and plan, severe bipolar mania, and severe eating disorders need hospital-level care first. Second, where the indicated treatment is long-term schema therapy or another modality we do not offer in-house, we will say so at the assessment stage and recommend the right pathway rather than pretend we cover everything.
If you or someone you love is struggling with substance dependence, explore how a comprehensive drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
The most common questions about therapy choices in dual diagnosis treatment.
Neither is universally better — they treat different problems. CBT is first-line when the dominant issue is distorted thinking driving the substance use, typically in depression and anxiety presentations. DBT is first-line when emotional dysregulation is the dominant issue — borderline traits, self-harm history, suicidality. Most clients receive elements of both, with the proportion adjusted to the case.
Typically three to four modalities are used for one client, not the full menu. A common mix is CBT for thinking work, DBT skills for emotion regulation, motivational interviewing running through individual sessions, and group therapy. EMDR is added when trauma is a driver, family work is added when the family system is part of the picture.
EMDR involves bringing trauma memories deliberately into awareness for reprocessing. Doing this during early withdrawal — when the nervous system is already overwhelmed — typically makes symptoms worse and can drive relapse. Stabilisation work comes first: detox if needed, sleep restoration, grounding skills, sometimes medication adjustment. EMDR usually begins around week three or four, once the client can tolerate the material.
Trauma-Focused CBT is a distinct structured protocol — not just CBT applied to trauma. It places the trauma narrative at the centre of treatment, builds tolerance for the material through gradual exposure, and reframes the meanings the client has attached to the event. Regular CBT addresses thinking and behaviour broadly; TF-CBT and EMDR are the two trauma-specific evidence-based options.
Not as a primary modality. Schema therapy is a long-term treatment, typically running over a year or more, which does not fit residential timeframes. We use schema-informed elements within DBT and individual therapy where relevant. If full schema therapy is the indicated treatment, we recommend completing residential stabilisation and substance use work with us, then continuing schema therapy with a specialist outpatient clinician afterwards.
Both. MI can be delivered as a short standalone intervention — typically when the goal is moving someone from contemplation into action — but in residential dual diagnosis it usually runs as a conversational style woven through every individual session. A skilled therapist using MI does not lecture or persuade; they elicit the client’s own reasons for change and amplify them.
The visiting consultant psychiatrist assesses at intake, prescribes or adjusts medication during the stay, and coordinates with the therapy team through case reviews. Most psychiatric medications take four to six weeks to reach full effect, so changes are made on a clinical timeline rather than a programme timeline. The medication itself is billed separately from the programme fee.
Written by
Alastair Mordey
Alastair Mordey is one of the pioneers of drug and alcohol treatment globally and specifically in Asia. He has been an addiction’s professional for twenty years. He started his career as an expert in substance abuse w...
Learn more about Alastair
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn








