Key Takeaways
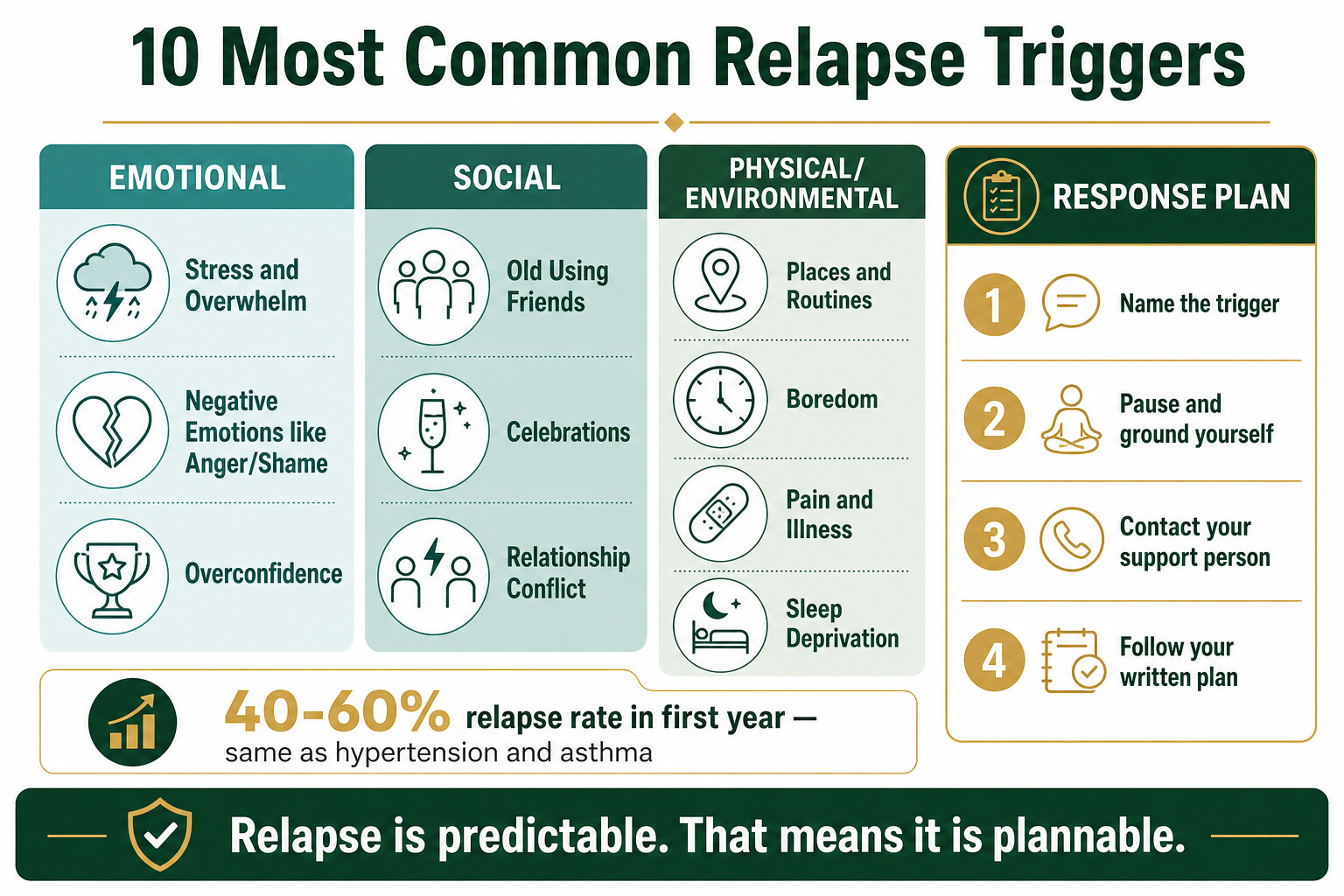
- Relapse happens in 40-60% of people treated for addiction — roughly the same rate as relapse in hypertension and asthma. It’s a sign the plan needs adjusting, not that treatment failed.
- The 10 most common triggers fall into three categories: emotional (stress, negative feelings, overconfidence), social (old using friends, celebrations, relationship conflict), and physical (environmental cues, boredom, pain, poor sleep).
- Each trigger has a specific, practical counter-strategy you can write into a relapse prevention plan before you leave treatment — not vague advice, but concrete actions for concrete situations.
- Environmental cues (places, objects, routines linked to past use) are among the strongest triggers: a meta-analysis of 237 studies found they more than double the odds of relapse.
- Residential treatment gives you a window to rehearse trigger responses in a controlled setting — the longer you practise, the more automatic those responses become in the real world.
Between 40% and 60% of people relapse within the first year after addiction treatment — a rate almost identical to other chronic conditions like hypertension and asthma (NIDA, 2024). That statistic isn’t meant to discourage you. It means relapse is predictable, which means it’s plannable. The people who stay in recovery aren’t the ones who white-knuckle it — they’re the ones who identified their specific triggers before discharge and built a written plan for each one.
This post breaks down the 10 triggers we see most often in residential clients, explains why each one works the way it does, and gives you a concrete response plan you can start building today.
Why Is Relapse So Common After Addiction Treatment?
Relapse is common because addiction changes how the brain responds to stress, reward, and environmental cues — and those changes don’t fully reverse when treatment ends. NIDA classifies addiction as a chronic, relapsing condition comparable to diabetes or heart disease, where returning symptoms signal a need to adjust treatment rather than abandon it (NIDA, 2024).
Marlatt and Gordon’s relapse prevention model — still the most widely used framework in clinical practice — identifies two layers that lead to relapse: immediate triggers (a fight with your partner, walking past your old bar) and background factors that make you vulnerable to those triggers (poor sleep, lifestyle imbalance, unmanaged stress) (Larimer et al., Alcohol Res Health, 1999). Understanding both layers is what separates a relapse prevention plan from wishful thinking.
A systematic review of 321 studies found that the most consistent predictors of relapse were psychiatric comorbidity, craving intensity, and lack of social support — while protective factors included self-efficacy, supportive networks, and a sense of purpose (Sliedrecht et al., Drug Alcohol Depend, 2019). All 10 triggers below map onto these evidence-based risk factors.
| Trigger | Category | Core Response |
|---|---|---|
| 1. Stress and overwhelm | Emotional | Recognise early signs, activate coping plan before crisis |
| 2. Negative emotions (anger, shame, sadness) | Emotional | Name the emotion, use a grounding technique, call your support person |
| 3. People from your using days | Social | Set boundaries before you need them — have exit scripts ready |
| 4. Places and routines linked to past use | Environmental | Map your high-risk locations, plan alternative routes and routines |
| 5. Celebrations and positive events | Social | Decide what you’ll drink and say before the event starts |
| 6. Boredom and unstructured time | Environmental | Schedule your week — empty hours are the enemy |
| 7. Relationship conflict | Social | Pause before reacting, use “time-out” agreements with partner/family |
| 8. Physical pain or illness | Physical | Tell every doctor about your addiction history — have a medication safety plan |
| 9. Sleep deprivation and exhaustion | Physical | Protect sleep like a medical prescription — it is one |
| 10. Overconfidence | Emotional | Treat “I’ve got this” as a warning sign, not proof of recovery |
How Do Stress and Negative Emotions Trigger Relapse?
Stress is the single most researched relapse trigger in addiction science. Chronic stress disrupts the brain’s normal stress-response system, making people in early recovery hyper-reactive to everyday pressures that non-addicted people handle without thinking. Research from Yale’s Stress Center found that stress-induced craving — not just exposure to drug cues — predicted both shorter time to relapse and higher amounts of substance use after treatment (Sinha, J Clin Med, 2024).
Trigger 1: Stress and Overwhelm
Work deadlines, financial pressure, family conflict, legal problems — the stress doesn’t disappear when you leave rehab. What changes is your ability to handle it without substances. The danger period is the first 90 days, when your new coping skills are still fragile and your old ones (using) are deeply wired.
Your plan: Write down your top three stress sources before discharge. For each one, write a specific action — not “manage stress better” but “when I feel overwhelmed at work, I will walk outside for 10 minutes and call my sponsor before making any decisions.” Practise this in therapy sessions so the response becomes automatic.
Trigger 2: Negative Emotions (Anger, Shame, Sadness, Loneliness)
Many people used substances specifically to numb difficult emotions. In recovery, those emotions come back — sometimes with interest. Shame about past behaviour, anger at yourself or others, grief for lost relationships or wasted years. Marlatt’s research found that negative emotional states were the most frequently reported trigger across all substance types (Larimer et al., Alcohol Res Health, 1999).
Your plan: Learn to name emotions with specificity. “I feel angry because my brother didn’t call” is manageable. “I feel bad” is not — it leaves you with a vague discomfort and no clear action. Techniques like CBT and DBT give you structured ways to identify emotional triggers before they escalate into cravings.

Why Are People and Places From Your Past So Dangerous?
Environmental cues — the people, places, and objects your brain associates with drug use — are among the most powerful relapse triggers known to science. A meta-analysis of 237 studies involving over 51,000 participants found that exposure to drug-related cues more than doubled the odds of future drug use or relapse (Vafaie & Kober, JAMA Psychiatry, 2022). Your brain doesn’t forget where it got high — and it won’t ask permission before sending a craving.
Trigger 3: People From Your Using Days
Old drinking buddies, a dealer’s phone number still in your contacts, friends who still use. These aren’t bad people, but being around them activates the same neural pathways that drove your addiction. The social pressure can be obvious (“just one drink”) or subtle (just being in their company makes using feel normal again).
Your plan: Before you leave treatment, make two lists: people who support your recovery and people who threaten it. Delete phone numbers. Prepare specific responses for unexpected encounters — “I’m not drinking anymore, and I need to head out” is enough. You don’t owe anyone an explanation. Build new social connections through recovery groups, fitness, or activities that don’t involve substances.
Trigger 4: Places and Routines Linked to Past Use
The bar you used to drink at, the route you drove to pick up, even your own kitchen at 10pm on a Friday. Context-dependent memory means these places can trigger cravings even months after your last use. Research on drug-associated contexts shows that environments reliably paired with drug use can reignite extinguished drug-seeking behaviour even after prolonged abstinence (Vafaie & Kober, JAMA Psychiatry, 2022).
Your plan: Map your high-risk locations before discharge. Plan alternative routes home. Change routines: if Friday nights were your trigger, schedule something incompatible — a gym session, a recovery meeting, dinner with a sober friend. For unavoidable environments (your own home), physically rearrange the space. Move furniture, clear out anything associated with using, change the lighting. It sounds trivial, but disrupting the visual cues genuinely helps.

Can Celebrations and Good Times Cause Relapse?
Yes — and this catches people off guard because they’ve only prepared for negative triggers. Celebrations, promotions, holidays, weddings, and even just a good day can trigger relapse because your brain associates reward with substances. The feeling of “I deserve to celebrate” or “one drink won’t hurt on a night like this” bypasses the rational defences you’ve built for bad days.
Positive emotional states accounted for a significant portion of relapse episodes in Marlatt’s research — people who’d stayed sober through difficulty relapsed at a party because they hadn’t planned for feeling good (Larimer et al., Alcohol Res Health, 1999).
Your plan: Before any social event, decide three things: what you’ll drink (have a specific non-alcoholic option — not “I just won’t drink”), what you’ll say if offered a drink, and when you’ll leave. Bring your own car so you’re not dependent on someone else’s timeline. Tell at least one person at the event that you’re not drinking — accountability removes the temptation to quietly change your mind. If you’ve been through alcohol withdrawal before, remembering what that felt like can be a powerful deterrent when someone offers you that first drink.
Want help building a trigger plan that’s specific to your situation? Talk to our team — we’ll give you a straight answer about what treatment looks like.
Why Is Boredom One of the Biggest Relapse Risks?
Boredom is one of the most underestimated relapse triggers because it doesn’t feel like a crisis — it feels like nothing. But that’s exactly the problem. Unstructured time leaves space for cravings to grow, and without an alternative activity, your brain defaults to the behaviour that used to fill the gap. In residential treatment, every hour is scheduled. The transition to an open diary is where many people stumble.
Your plan: Build a weekly schedule before you go home. Not a vague “stay busy” intention — an actual timetable with specific activities in specific time slots. Fill high-risk times first (evenings, weekends, time alone). Exercise, meetings, volunteer work, hobbies you dropped during active addiction. The schedule from your time in treatment gives you a template — adapt it for home life. Some of our clients find that the activities they tried during treatment — Muay Thai, hiking, yoga — become long-term replacements for the time they used to spend using.

How Do Relationship Problems Trigger Relapse?
Interpersonal conflict is a relapse trigger with strong research backing. Arguments with a partner, family tension, feeling rejected or unsupported — these create the kind of acute emotional pain that substances used to numb. Research shows that people with high sensitivity to rejection and those in critical interpersonal environments face particular vulnerability to relapse, because social pain activates the same brain pathways as physical pain (Cornelius et al., Addict Behav, 2014).
Your plan: Set up “time-out” agreements with your partner or close family before conflict happens. The agreement: when an argument escalates past a certain point, either person can call a pause — no guilt, no accusation. You separate for 30 minutes, use a grounding technique, and return to discuss when you’re calmer. If relationships are a primary trigger, couples or family therapy during treatment gives you communication tools you can carry home. This isn’t about avoiding conflict — that’s impossible — it’s about having a protocol for when it happens.
How Do Pain, Illness, and Exhaustion Increase Relapse Risk?
Physical discomfort and fatigue lower your defences in measurable ways. When your body is struggling, the executive control functions in your prefrontal cortex — the same ones you rely on to resist cravings — are impaired. This is biology, not weakness.
Trigger 8: Physical Pain or Illness
Dental work, a back injury, post-surgical pain — these situations put people in direct contact with the medical system and potentially with prescription opioids or other addictive medications. For someone with a substance use history, a routine prescription can be the start of a relapse.
Your plan: Tell every healthcare provider about your addiction history. This isn’t optional — it’s as important as telling them about a drug allergy. Ask about non-addictive pain management options first. If opioids are truly necessary (some situations require them), have someone else hold the medication and dispense it on schedule. Write these instructions in a card you carry in your wallet: “I am in recovery from substance addiction. Please discuss non-opioid pain management options with me first.”
Trigger 9: Sleep Deprivation and Exhaustion
Sleep disruption is present in over 75% of people with substance use disorders, and a growing body of research shows that reduced sleep directly increases vulnerability to relapse. Animal studies have demonstrated that both sleep restriction and sleep deprivation increase preference for alcohol and cocaine self-administration (López-Muciño et al., Neurosci Biobehav Rev, 2022). In human studies, poor sleep predicts craving intensity and relapse timing.
Your plan: Treat sleep hygiene like a medical prescription. Fixed wake time every day (including weekends). No screens for an hour before bed. No caffeine after 2pm. Exercise daily, but not within three hours of bedtime. If insomnia persists beyond a few weeks in recovery, see a doctor — untreated sleep problems are a genuine relapse risk, not something to tough out. During treatment at One Step, our daily schedule is built around consistent wake times and physical activity partly because it resets sleep patterns that addiction destroyed.
Relapse triggers are not a mystery — they follow predictable patterns. What I see with clients who stay in recovery is that they identified their personal triggers during treatment and rehearsed their responses until those responses became reflexive. The ones who relapse are usually the ones who assumed they’d figure it out when the moment came.
David KaffSenior Therapist, One Step Rehab
What Makes Overconfidence the Sneakiest Trigger?
Overconfidence — the belief that you’ve beaten addiction and can safely test your limits — is arguably the most dangerous trigger because it disguises itself as progress. “I can have just one.” “I’m strong enough now.” “It’s been six months — I’m past the danger zone.” These thoughts feel like evidence of recovery, but they’re actually the setup for relapse.
In Marlatt’s model, this is called the “abstinence violation effect” — the gap between your confidence and your actual coping capacity. When someone tests their limits and fails, the resulting shame often accelerates a full relapse rather than just a single lapse (Larimer et al., Alcohol Res Health, 1999).
Your plan: Treat the thought “I can handle it now” as a red flag, not a green light. When it shows up — and it will — call your sponsor, your therapist, or a trusted friend immediately. Not after you’ve acted on it. The rule is simple: if you’re thinking about whether you can safely use, you cannot. Overconfidence typically peaks at 3-6 months of sobriety, when the pain of active addiction has faded but the neural pathways are still intact. Stay in your aftercare programme through this window — it exists precisely for this reason.

How Does One Step Rehab Prepare Clients for Real-World Triggers?
Every client at One Step builds a personalised trigger map during their stay — not a generic worksheet, but a document based on their actual history, their actual high-risk situations, and the specific responses they’ve rehearsed in individual and group therapy sessions. Here’s how that works in practice.
Structured daily programme: Our treatment programme runs on a fixed schedule — morning meditation, breakfast, group therapy, individual sessions, fitness, evening reflection. This structure isn’t arbitrary. It teaches your brain to operate on a predictable routine, which is the single most effective defence against boredom and unstructured-time triggers when you return home.
CBT and DBT sessions: Cognitive behavioural therapy and dialectical behaviour therapy are the core of our therapeutic approach. CBT helps you identify the thought patterns that precede cravings (“I deserve a break” → “I deserve a drink”). DBT gives you emotional regulation tools for the intense feelings — anger, shame, loneliness — that drive impulsive decisions.
Physical activity as trigger replacement: Muay Thai, gym sessions, hiking, yoga — these aren’t luxury extras. Exercise produces natural dopamine, reduces stress hormones, improves sleep, and fills the hours that used to be occupied by using. Clients who leave with an exercise habit have a concrete boredom-and-stress coping tool that doesn’t require a meeting or a phone call. Pairing regular exercise with a nutrition plan that supports dopamine recovery strengthens both effects.
Aftercare: Trigger planning doesn’t end at discharge. Our aftercare programme provides ongoing check-ins to monitor how your trigger plan holds up against real life. When new triggers emerge — and they will — aftercare gives you a place to update your plan with professional support.
What it costs: One Step charges ฿280,000/month (~$8,500 USD). That covers accommodation, all therapy sessions, meals, fitness activities, and aftercare. Medication prescribed by the doctor is billed separately — like flights, visas, and personal items. See the full breakdown on our pricing page.
If you or someone you love is struggling with substance dependence, explore how a structured drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions About Relapse Triggers
Quick answers to the most common questions about relapse triggers and prevention planning.
Stress and negative emotional states are the most frequently reported relapse triggers across all substance types. Research consistently ranks them above environmental cues and social pressure, though all three categories interact. The key is identifying which specific form of stress — financial, relational, professional — affects you most, and building a response plan for that scenario.
The first 90 days after treatment carry the highest relapse risk, with acute vulnerability in the first 30 days. However, overconfidence often peaks at 3-6 months, creating a secondary danger window. This is why aftercare programmes that extend beyond the initial treatment period significantly improve long-term outcomes.
No plan guarantees zero relapse, and anyone promising that is not being honest. What a strong relapse prevention plan does is reduce the frequency and severity of relapse episodes and, critically, help you respond to a lapse before it becomes a full relapse. NIDA frames addiction as a chronic condition where relapse signals a need to adjust treatment — not that treatment has failed.
Yes. Research consistently shows that treatment duration is one of the strongest predictors of sustained recovery. NIDA recommends a minimum of 90 days for residential treatment. At One Step, most clients stay 28-60 days, and we’re upfront that shorter stays rarely produce lasting change. The more time you spend practising trigger responses in a controlled environment, the more automatic they become.
Stop using immediately, call your sponsor or therapist, and be honest about what happened. A single lapse doesn’t have to become a full relapse. The biggest mistake people make is treating a lapse as proof of failure and giving up entirely. Analyse what triggered it, update your prevention plan, and re-engage with your support network. If needed, return to treatment — coming back is not a failure, it’s a recalibration.
The core triggers — stress, environmental cues, negative emotions, social pressure — are consistent across substances. What varies is the intensity and relative ranking. Alcohol relapse is more heavily driven by social situations and celebrations. Opioid relapse is more closely tied to physical pain and medical encounters. Stimulant relapse often connects to boredom and energy-seeking. Your trigger plan should reflect your specific substance history.
Yes. Relapse prevention planning is built into the treatment programme from week one. Clients work with their therapist to identify personal triggers, rehearse coping responses in individual and group sessions, and build a written plan they take home at discharge. The aftercare programme continues this work with regular check-ins after you leave.
Written by
David Kaff
David Kaff is an Addictions Counselor with over a decade of experience working in both harm reduction and residential treatment settings in Australia and Thailand. He has worked across frontline services, 12-step based r...
Learn more about David
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn