
Key Takeaways
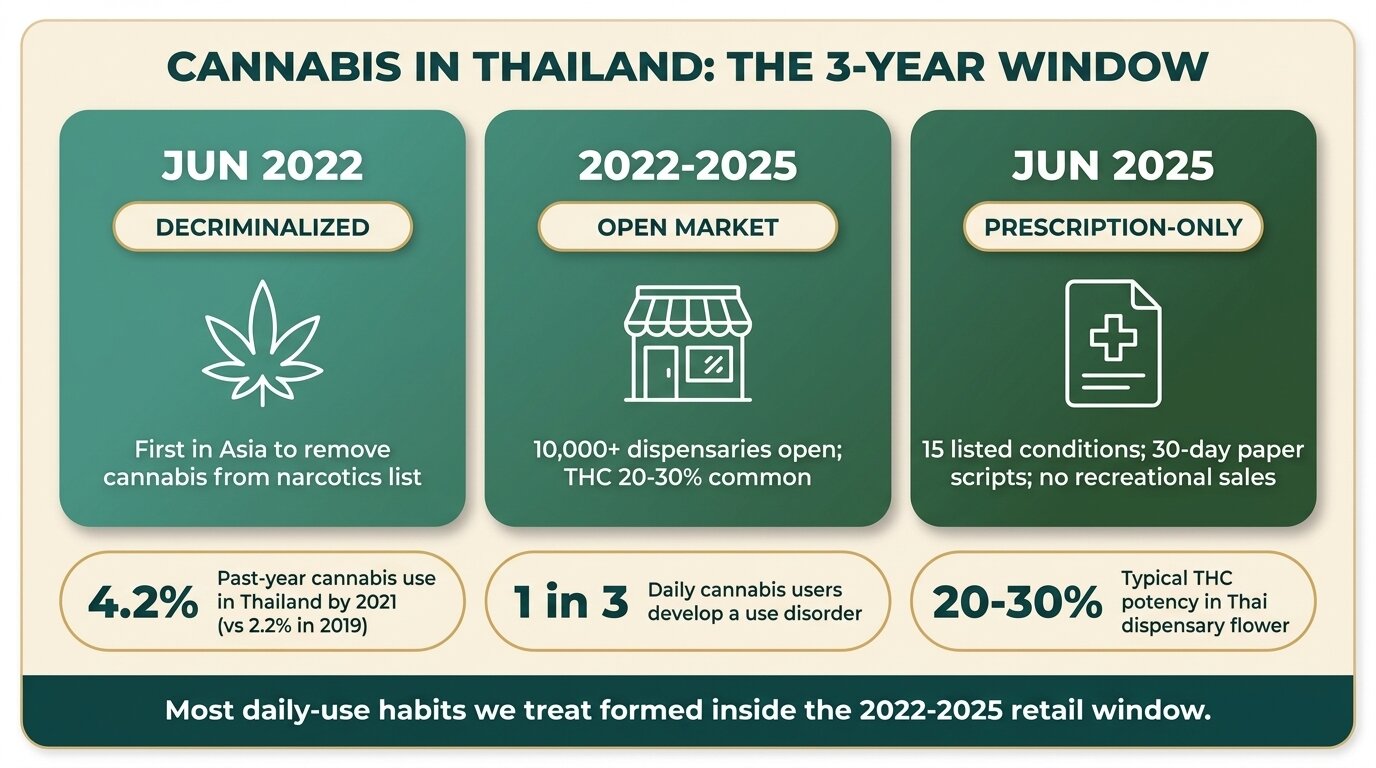
- Thailand removed cannabis from its narcotics list on 9 June 2022, then reversed course on 25 June 2025 — recreational sales are now banned and cannabis is sold by prescription only for 15 listed conditions.
- Thai dispensary cannabis routinely tests at 20-30%+ THC, several times stronger than the imported street weed Thailand had before 2022 — and high-potency cannabis is the form most strongly linked to addiction and psychosis.
- Cannabis use disorder is a real DSM-5 diagnosis. Roughly 1 in 10 cannabis users develop dependence; the rate rises to about 1 in 6 for people who start before 18 and 1 in 3 for daily users.
- Cannabis hyperemesis syndrome (CHS) — repeat cycles of severe vomiting in chronic daily users — has risen sharply at hospitals in legalised markets and is now being reported across Thailand.
- One Step Rehab in Chiang Mai treats cannabis use disorder as part of our 28-day residential programme at ฿280,000/month (~$8,500 USD). Cannabis withdrawal is uncomfortable but not medically dangerous — we manage it on-site.
Cannabis addiction in Thailand is real, clinically recognised, and more common than people think. About 9-10% of cannabis users develop a cannabis use disorder, rising to roughly one in three among daily users (StatPearls, NIH, 2026). After Thailand’s June 2022 decriminalisation, daily cannabis use here became cheap, social, and culturally normal almost overnight — and the product on sale at Thai dispensaries is far stronger than what most users grew up with. The June 2025 prescription-only rules changed the legal status of the market, but they didn’t shrink the population of people who’d developed a daily habit.
This piece is for three people: the expat in Chiang Mai who has been smoking after work every day for two years and isn’t sure if that’s a problem; the traveller who started using on holiday and can’t seem to stop now they’re home; and the parent of a 22-year-old who came to Thailand for “a few months” and is still here, mostly stoned. We’ll cover what actually happened with Thai cannabis policy, what the clinical picture looks like, and when professional treatment is worth considering.
What Actually Happened With Cannabis in Thailand (2018-2025)?
Thailand became the first country in Asia to remove cannabis from its narcotics list on 9 June 2022, championed by then-Health Minister Anutin Charnvirakul of the Bhumjaithai Party (Yimsaard et al., Lancet Reg Health Southeast Asia, 2023). On 25 June 2025, the Public Health Minister reversed course: prescription-only sales, no recreational use, and a draft bill to re-add cannabis flower to the narcotics list.
The full timeline matters because it explains why so many people developed daily habits here in such a short window.
| Date | What changed | Practical effect |
|---|---|---|
| 2018-2019 | Medical cannabis legalised | Tightly controlled, used only in licensed clinics |
| 9 June 2022 | Cannabis removed from Category 5 narcotics list | Plant, flower, and extracts (under 0.2% THC officially) became legal to grow, sell, and possess |
| Late 2022 – 2024 | No comprehensive control law passed | Legal grey zone: over 10,000 dispensaries opened nationally; tourist-area cafés in Bangkok, Chiang Mai, Phuket; THC limits unenforced in practice |
| 2024 | Pheu Thai government announces intent to recriminalise | Industry uncertainty; tourists and locals still buying freely |
| 25 June 2025 | Public Health Ministry order: prescription-only sales | Buyers need a paper prescription from a licensed practitioner, valid for 30 days, for one of 15 listed conditions (cancer, chronic pain, asthma, depression, others) |
| 2025-2026 | Draft bill to re-list cannabis as a narcotic | Many dispensaries closed; others operate through clinic partnerships; black-market sales continue |
The 2022-2025 window — three years of essentially unregulated retail — is when most of the daily-user habits we now see at clinics took shape. Past-year cannabis use in Thailand rose from 2.2% in 2019 to 4.2% in 2021, and continued climbing after the 2022 decriminalisation (Kalayasiri et al., BMC Public Health, 2023). For 18-19 year olds, the figure more than doubled in the same period.
Why Is Thai Dispensary Cannabis So Much Stronger Than Old Street Weed?
The cannabis sold in Thai dispensaries since 2022 routinely tests at 20-30% THC, with some concentrates above 70%. The street cannabis circulating in Thailand and across Asia in the 1990s averaged around 3-5% THC. That’s a 5-10x potency jump in a single generation, and high-potency cannabis is consistently associated with higher rates of cannabis use disorder and psychosis (Annals of Internal Medicine, 2025).
People often assume cannabis is cannabis — “I smoked weed in college and was fine, so my kid will be fine.” That’s no longer a safe assumption. Modern indoor-grown, selectively bred strains, plus rosin, shatter, and vape carts, deliver THC doses per session that simply weren’t available 20 years ago.
| Product | Typical THC content | What it means for a daily user |
|---|---|---|
| 1990s imported street weed | 3-5% | Low ceiling on dose per session |
| Mid-2000s commercial flower | 8-12% | Noticeable tolerance build-up over months |
| Thai dispensary flower 2024 | 20-30% | Tolerance and withdrawal develop within weeks of daily use |
| Thai dispensary concentrates (rosin, shatter) | 60-90% | Each session delivers a multi-day dose by old standards |
| Vape cartridges | 70-90% | Easy to use through the workday; harder to track total intake |
This isn’t moralising about cannabis. Many people use it occasionally and without harm. The point is narrower: if you started using daily-strength dispensary product after moving to Thailand, what you’re using is not the cannabis you remember from your teens or twenties, and the dose-response data tells us higher potency raises addiction risk in a fairly linear way.
Is Cannabis Addiction Actually Real?
Yes. Cannabis use disorder is in the DSM-5 — the diagnostic manual psychiatrists use globally — and it’s diagnosed using the same impairment framework as alcohol or cocaine use disorder. About 9-10% of all cannabis users develop the disorder; the rate climbs to roughly 1 in 6 for people who start before 18, and around 1 in 3 for daily users (StatPearls, NIH, 2026).
The most common pushback we hear from clients in their first week is some version of: “Weed isn’t addictive — that’s a myth from the war on drugs.” It’s worth separating that political point from the clinical one. Cannabis withdrawal is real and well-documented. Daily users who stop typically get poor sleep, anxiety, irritability, vivid dreams, sweating, and reduced appetite for 1-2 weeks (Bonnet & Preuss, Subst Abuse Rehabil, 2017). It’s not life-threatening like alcohol or benzodiazepine withdrawal — but it’s bad enough that people relapse to relieve it, which is how dependence works.
The DSM-5 criteria for cannabis use disorder are the questions most users find hardest to honestly answer. You meet the diagnosis if two or more of these apply over a 12-month period:
- Using more, or longer, than you intended
- Wanting to cut down and not being able to
- Spending a lot of time getting it, using it, or recovering from it
- Cravings
- Missing work, school, or family obligations because of use
- Continuing despite social or interpersonal problems caused by it
- Giving up activities you used to value
- Using in situations where it’s physically risky (e.g. driving)
- Continuing despite knowing it’s making a physical or mental problem worse
- Tolerance (needing more for the same effect)
- Withdrawal when you stop
Two to three is a mild disorder. Six or more is severe. People are often surprised to find they tick seven.
What Is Cannabis Hyperemesis Syndrome — And Why Is It Showing Up in Thai Hospitals?
Cannabis hyperemesis syndrome (CHS) is a condition that develops in some long-term, heavy cannabis users — typically after years of daily use. It causes cycles of severe nausea, repeated vomiting, and abdominal pain that hot showers temporarily relieve. CHS hospitalisations have risen sharply in legalised markets, and Thai emergency departments have seen the same pattern since 2022 (Marshall et al., J Clin Gastroenterol, 2024).
This is the diagnosis most cannabis users actively resist, because the relationship between the symptom and the cause is so counterintuitive: the drug they’re using to feel better (and that has antiemetic properties medically) is the thing making them violently sick. People often spend years cycling through ER visits, GI workups, and abdominal CT scans before someone asks how much they smoke (Stubbs et al., J Investig Med, 2024).
Classic CHS presentation:
- Years of daily, heavy cannabis use (almost always required)
- Recurrent episodes of severe vomiting, often 1-2 days at a time
- Diffuse abdominal pain
- Compulsive hot showers or baths for symptom relief — the single most distinctive feature
- Symptoms fully resolve only when the person stops using cannabis
At One Step we’ve started seeing CHS as a presenting complaint in the assessment call, not just an incidental finding. If you’re showering five times a day to stop vomiting, that’s not normal — and it’s not going to get better while you keep smoking.
Most of the cannabis cases we see now would have been considered unusual ten years ago. They’re daily users on 20%-plus THC flower or vape carts, not the occasional joint smoker. The withdrawal isn’t dangerous the way alcohol or benzo withdrawal is — nobody’s going to seize — but it’s miserable enough that people give up and go back. That’s the cycle treatment breaks.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Who Should Actually Worry About Their Use?
Not every cannabis user has a problem. The reasonable test is functional, not moral: is daily use changing how your life works in ways you don’t want? The signs that the line has been crossed are consistent across the people we treat — and they’re rarely about volume alone.
Not sure if your use is a problem yet? Talk to our team — we’ll give you a straight answer over a confidential call, even if our programme isn’t right for you.
The three cohorts most likely to need treatment, in our experience running residential programmes:
The expat who normalised daily use. Moved to Chiang Mai, Bangkok, or Phuket between 2022 and 2025. Started smoking with friends, then alone after work, then through the day. Hasn’t taken a break longer than a weekend in months. Sleep is wrecked without it. Productivity is sliding. Says “I can quit any time” but each attempt lasts 2-4 days.
The traveller who can’t put it down at home. Came on holiday, discovered Thai dispensaries, came back with vape carts or established a re-supply route. Six months later, daily use, secrecy at home, anxiety when running low. This pattern is common with stimulants and is now common with high-potency cannabis too.
The 18-25 year old whose parents are worried. Studying or “taking a year out” in Thailand. Daily use started in the first month. Now socially withdrawn, sleeping until afternoon, not engaging with the original plan for the time abroad. Cannabis at this age is associated with measurably higher rates of psychiatric illness, including psychosis (Annals of Internal Medicine, 2025) — the brain is still developing until the mid-20s.

How One Step Treats Cannabis Use Disorder
One Step Rehab runs a 28-day residential programme in Chiang Mai for ฿280,000/month (~$8,500 USD). For cannabis use disorder we treat on-site — there’s no severe withdrawal that needs hospital-level care, and most clients are physically off cannabis within the first week. The work isn’t the withdrawal; it’s rebuilding a life that doesn’t run on it.
What our cannabis clients can expect during their stay:
- Days 1-3: Sleep disruption peaks, irritability, sweating, vivid dreams, low appetite. We use sleep hygiene structure, light medication if the psychiatrist prescribes it (medication is billed separately), and an early morning schedule to reset the body clock.
- Days 4-14: Mood and anxiety symptoms peak around day 6-7 and then start to lift. Group therapy, individual counselling, and CBT-based work begins. We use the CBT and DBT frameworks our team is trained in for cravings and emotional regulation.
- Weeks 3-4: Withdrawal is largely over. Work focuses on what the cannabis was actually doing — managing anxiety, social discomfort, sleep, boredom — and what replaces it. Activities (Muay Thai, hiking, swimming, yoga) carry significant weight here, because most clients have lost any non-substance way to wind down.
- Aftercare: Structured aftercare for the first 90 days post-discharge, which is when most cannabis relapses happen. Sleep often takes 6-8 weeks to fully normalise, and that’s when people get tempted back.
What’s included in the fee: accommodation, food, group and individual therapy, intake assessment, routine progress checks with our visiting psychiatrist, activities, and transport for programme-related trips. What’s not included: medication prescribed by the doctor, additional counselling beyond the standard schedule, hospital visits, flights, visa fees, and personal items. See the full pricing breakdown.
For more on our overall structure, see our treatment programme page and daily schedule. The cannabis rehab landing page covers admission specifics.

What Should You Do Now If You Think You Have a Problem?
If two or more of the DSM-5 criteria above apply to you, you have at least a mild cannabis use disorder by clinical definition. That doesn’t automatically mean residential treatment — but it does mean self-managing isn’t the obvious right answer either. The decision tree is fairly simple in practice.
| Situation | Reasonable first step |
|---|---|
| Daily use under 12 months, no co-occurring mental health issues, supportive home environment | Try a 30-day break with support: an accountability partner, no cannabis at home, scheduled exercise. If you can’t get past day 4-5, escalate. |
| Multiple failed quit attempts, anxiety or depression alongside, daily use for 1+ year | Outpatient counselling with someone who works in substance use specifically. Not a generalist. |
| Daily heavy use of high-potency product, CHS symptoms, social or work decline, can’t function without it | Residential treatment. The first 2 weeks off cannabis are when most attempts fail without environmental change. |
| Cannabis-induced psychosis or panic attacks, suicidal thinking, prior psychiatric history | Psychiatric assessment first. Dual diagnosis treatment if both conditions need addressing. |
If you’re in Thailand currently, the prescription-only rules mean your supply route is now uncertain in a way it wasn’t before. For some people that’s a useful forcing function: the addiction has already done what it’s going to do, and the constraint of needing a prescription is an opportunity to stop. For others it just means the source moves underground. Either way, the clinical question — am I dependent? — doesn’t change.
Frequently Asked Questions
Common questions from people considering whether their cannabis use has become a problem.
Cannabis use disorder is a recognised DSM-5 diagnosis used by psychiatrists worldwide. About 9-10% of all cannabis users develop it, rising to roughly 1 in 3 daily users. The “not addictive” framing usually comes from comparing cannabis to opioids or alcohol — it’s lower-risk than those, but that’s not the same as zero risk.
Only with a paper prescription from a licensed practitioner, for one of 15 listed medical conditions, valid for 30 days. Recreational sales were banned on 25 June 2025. Many dispensaries have closed or now operate through clinic partnerships; some continue informally but the legal exposure has changed significantly.
The acute physical symptoms — sleep disruption, irritability, sweating, vivid dreams, low appetite — typically peak between days 2-6 and largely resolve within two weeks. Sleep can take 6-8 weeks to fully normalise. Psychological cravings can persist for months, particularly in situations the brain has paired with cannabis use.
CHS is a cycle of severe vomiting, abdominal pain, and compulsive hot-shower seeking that develops in some long-term heavy cannabis users. Hospitalisations have risen sharply in legalised markets including Thailand since 2022. It only resolves when the person stops using cannabis — it’s the clearest evidence that cannabis can cause physical harm in dependent users.
No. Cannabis withdrawal is uncomfortable but not medically dangerous, so we handle it on-site at One Step. You can stop using when you arrive. We use sleep structure, daily activity, and counselling to manage the worst of the first week, and medication if the visiting psychiatrist prescribes it.
The 28-day residential programme is ฿280,000/month (~$8,500 USD). That covers accommodation, food, the structured therapy programme, intake assessment, routine progress checks with the visiting psychiatrist, and programme activities. Medication, additional counselling sessions, flights, visa fees, and personal items are billed separately.
You can contact us directly — we work with families regularly, especially of clients in their 20s. We can talk through how to approach the conversation, what an admission would look like, and whether transport from elsewhere in Thailand is needed. We won’t make promises we can’t keep about getting them through the door; ultimately they have to choose to come.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








