
Key Takeaways
- Physical dependence is not addiction. Anyone on daily opioids for more than a few weeks will develop dependence — that is normal pharmacology, not a personal failing. Opioid use disorder is a separate diagnosis with specific behavioural criteria.
- Tolerance creeps quietly. The dose that worked at month three usually does not work at month nine, and chasing that relief with higher doses is the most common path from legitimate prescription to dependence.
- Opioid-induced hyperalgesia is real. Long-term opioids can amplify the original pain instead of treating it — a paradox that makes patients feel they need more of the drug to function.
- Cold-turkey withdrawal is unsafe at high doses. Stopping abruptly from chronic prescription opioid therapy carries real medical risks; a structured taper, ideally with clinical support, is the safe route.
- Pain and dependence need treating together. Stopping the opioid does not treat the underlying condition that started the prescription. Rehab works only when the pain plan is part of the recovery plan.
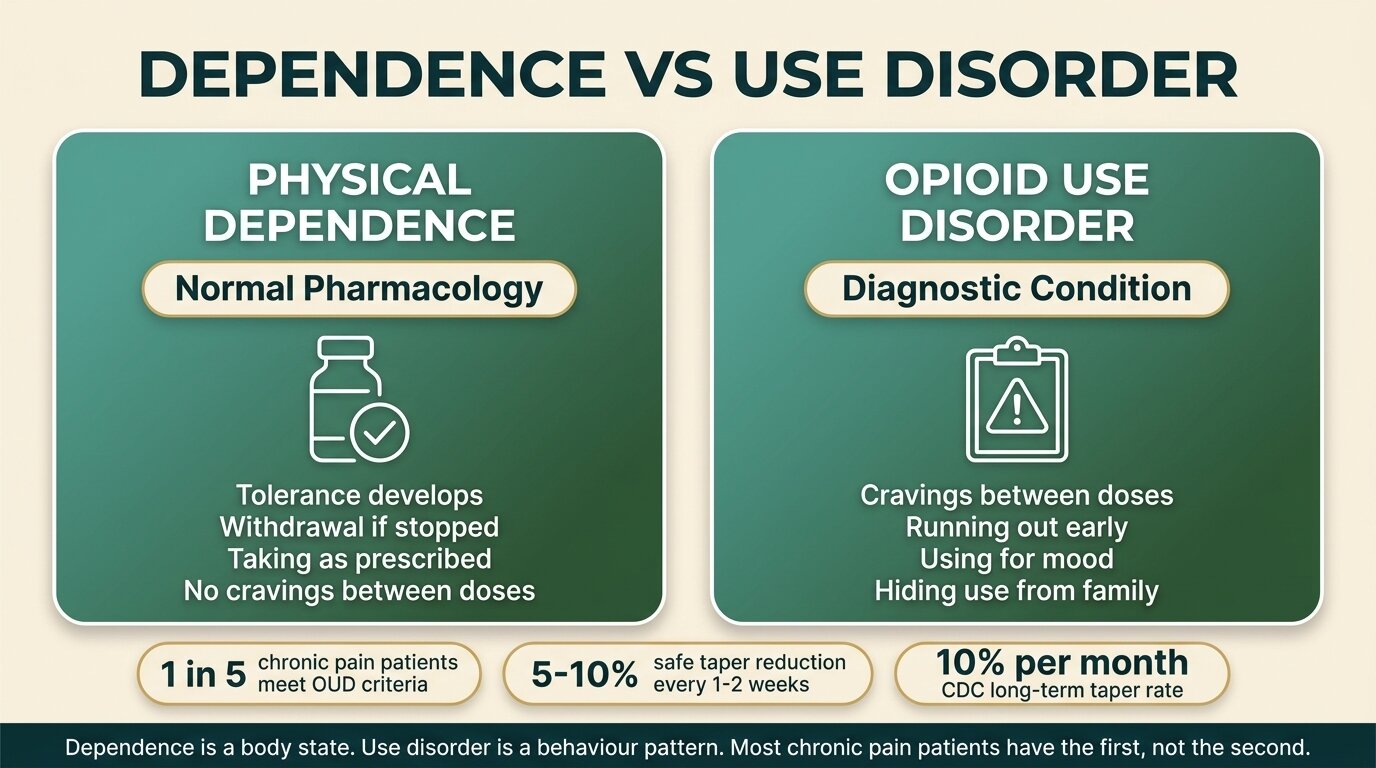
If you started taking opioids for a legitimate medical problem and now cannot stop without becoming ill, you are not an addict in the sense the word usually carries — you are physically dependent, and that distinction matters both medically and morally. Roughly one in five chronic pain patients on long-term opioid therapy meets criteria for opioid use disorder, but a much larger group sits in the awkward middle: dependent, struggling to taper, ashamed, and stuck between a prescriber who will not reduce the dose and a body that refuses to do without (Volkow & McLellan, N Engl J Med, 2016). This guide is for that group — the post-surgery, post-cancer, post-MVA, fibromyalgia, and chronic back-pain patients who never thought the word “rehab” applied to them, and now wonder if it might.
Is Physical Dependence the Same Thing as Addiction?
No. Physical dependence is a predictable adaptation — your body changes its chemistry to accommodate a drug, so removing it produces withdrawal. Opioid use disorder is a behavioural pattern: compulsive use despite harm, cravings, loss of control, neglecting responsibilities. You can have one without the other. Most long-term pain patients have dependence; a smaller subset has the full disorder.
The DSM-5, which is the diagnostic manual psychiatrists use, deliberately separates tolerance and withdrawal occurring under medical supervision from the criteria for opioid use disorder. A patient on stable, prescribed opioids who takes their medication exactly as directed and would experience withdrawal if it stopped does not, by that fact alone, have a use disorder. The disorder begins when behaviour drifts: taking extra doses on bad days, running out early, doctor-shopping, using to manage emotions rather than pain, hiding pill counts from your partner.
| Feature | Physical dependence only | Opioid use disorder |
|---|---|---|
| Tolerance | Yes — expected | Yes |
| Withdrawal if stopped | Yes — expected | Yes |
| Taking more than prescribed | No | Often |
| Cravings between doses | No | Yes |
| Running out early | No | Yes |
| Using for mood, not pain | No | Yes |
| Hiding use from family | No | Common |
| Continuing despite harm | No | Yes |
Why this matters: shame is a barrier to treatment. Patients who think “I am an addict” when they are actually dependent often avoid medical help because they cannot square that label with how they have lived their lives. Patients who recognise dependence as a physiological state — not a character verdict — get help sooner. The treatment, in both cases, eventually involves coming off the drug. The mindset you carry into that process is not a small detail.

Why Did the Same Dose Stop Working?
Tolerance is the most common reason a prescription opioid stops controlling pain over time. The opioid receptors in your brain become less responsive to the medication, so the dose that delivered relief at month three feels weak at month nine. Most patients then ask for an increase, get it, feel better briefly, and the cycle restarts. This is pharmacology, not weakness.
The clinical problem is what comes next. Each dose increase buys diminishing returns on pain control and steepens the slope of dependence. A systematic review of long-term opioid therapy for chronic pain found that the evidence for sustained pain relief and improved function beyond one year is weak, while evidence for serious harms — overdose, fractures, hormonal disruption, and abuse — increases with dose and duration (Chou et al., Ann Intern Med, 2015). The 2022 CDC clinical practice guideline makes the same point with stronger language: clinicians should avoid increases above 50 morphine milligram equivalents per day unless the benefit is clearly documented (Dowell et al., MMWR Recomm Rep, 2022).
The patient experience does not match the receptor biology. You feel like the pain is getting worse. The doctor says the imaging has not changed. Both can be true at once — the pain perception system itself becomes hypersensitive on long-term opioids, which brings us to the second mechanism almost nobody explains to patients.
What Is Opioid-Induced Hyperalgesia?
Opioid-induced hyperalgesia is when the painkiller starts amplifying pain instead of dulling it. The same nervous system that adapts to the drug also becomes more sensitive to pain signals — so patients report worse pain on higher doses, often spreading beyond the original injury. The fix is counter-intuitive: lowering the dose, slowly, often improves pain rather than worsening it.
This is not a fringe theory. A systematic review and meta-analysis of clinical populations after chronic opioid exposure found consistent evidence that long-term opioid use sensitises pain processing in ways that can be measured experimentally (Higgins et al., Br J Anaesth, 2019). A 2021 review describes the shared mechanisms — neuroinflammation and central sensitisation — that link chronic pain itself with hyperalgesia caused by the drug used to treat it (Santoni et al., Minerva Anestesiol, 2021).
For the patient, the practical sign of hyperalgesia is pain that does not match the injury anymore: pain at sites that were never injured, pain that spreads, pain that flares between doses and is only briefly soothed by the next pill. This pattern is often misread as “the underlying disease is getting worse, I need more medication” when in fact the medication is part of the cause. The only way to know which is happening is a carefully supervised taper — if pain improves as the dose comes down, hyperalgesia was contributing.

What If My Doctor Will Not Reduce the Dose?
You have three options, in roughly this order: ask for a written, paced taper plan from your prescriber; request a referral to a pain specialist or addiction medicine physician; or seek a structured residential setting where taper and pain management can happen together. Never stop or reduce a chronic opioid prescription on your own, especially at higher doses — that is where the medical risks become real.
Some prescribers refuse to taper because they were trained to under-treat pain, fear losing the patient, or have not kept up with the literature on long-term harms. Others refuse for the opposite reason — they are frightened of regulatory scrutiny and want to keep the patient stable on whatever dose has been working. Neither stance helps a patient who has decided they want off the drug. A polite, written request that specifies “I am asking for a slow taper, beginning with a 10% reduction over four weeks” lands better than a vague complaint.
If the prescriber still refuses, escalate. Pain medicine specialists, addiction medicine physicians, and physiatrists are usually more comfortable supervising a taper than primary-care doctors who started the prescription. In some cases the most realistic option is residential treatment — not because the dependence is severe enough to need it on its own, but because the chronic pain that started the whole thing makes outpatient tapering harder. Without an alternative pain plan in place, the first taper attempt usually fails.
Stuck between a prescriber who will not taper and a pain problem that has not gone away? Talk to our team — we will tell you honestly whether residential treatment fits your situation, and what other routes might.
Is Cold-Turkey Withdrawal Dangerous?
For high-dose chronic prescription opioid users, yes — abrupt cessation is genuinely unsafe and frequently catastrophic for any chance of recovery. Withdrawal itself is rarely fatal in otherwise healthy adults, but the rebound pain, dehydration, cardiac strain, and overwhelming distress drive most people back to opioids within days, often at the old dose. That post-detox relapse is where overdose deaths happen, because tolerance has dropped.
The CDC guidance is explicit on this: do not discontinue opioids abruptly in patients who have been on long-term therapy. A taper of 10% per month is a reasonable starting point for patients who have been on opioids for over a year, and slower for those on higher doses or with co-existing medical issues (Dowell et al., MMWR Recomm Rep, 2022). Patients with serious medical complications from their opioid dependence may need to begin the taper in a hospital setting before transferring to residential rehab — a small but important group whose situation is not safely handled in any outpatient programme.
Most of the people who arrive at our door from chronic pain prescriptions are not seeking a high and never were. They are seeking a way to live without the drug while still living with the pain. That is a different clinical problem from someone who became dependent recreationally, and it has to be treated differently — the taper has to be paced, the pain plan has to be real, and the shame has to be unpicked before anything else works.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab

How Does Rehab Handle Chronic Pain and Dependence at the Same Time?
A working programme treats them as one problem, not two. The opioid taper runs alongside an alternative pain plan — usually a combination of non-opioid medications, physical therapy, sleep correction, and psychological work on how pain is processed. Stopping the drug without replacing the pain management it was doing, however imperfectly, is the most common reason patients fail to stay off.
The components that matter, in roughly this order:
- Paced taper. Slow enough that withdrawal stays manageable. Reductions of 5-10% every one to two weeks are typical for someone who has been on prescription opioids for years.
- Alternative pain management. Non-opioid analgesics (paracetamol, NSAIDs where safe, certain antidepressants used for nerve pain, gabapentinoids in selected cases), physical therapy, posture and movement work, sleep correction, and sometimes interventional procedures done before admission.
- Psychological work on pain. Cognitive techniques that change how the brain processes chronic pain signals. Acceptance-based work for the pain that remains. CBT and related approaches are well-evidenced for both addiction and chronic pain.
- Shame work. The “I am not an addict” reflex has to be gently challenged without the patient feeling forced into a label they reject. Most clinicians settle on “you developed a medical problem from a medical treatment” — which is both accurate and unifying.
- Aftercare with an outside prescriber. Whoever picks up your prescriptions after rehab needs to know exactly what was tapered, what alternative medications are now in play, and what the pain plan looks like. Without this, the first bad pain flare-up sends people back to the original drug.
What Does One Step Do for Prescription-Opioid Patients?
At One Step Rehab in Chiang Mai, prescription-opioid clients with chronic pain follow our standard residential programme with three specific adjustments: the taper is paced individually rather than rushed, the visiting psychiatrist coordinates non-opioid pain management as the dose comes down, and the therapy work explicitly addresses the “I am not an addict” identity problem most of these clients arrive with. The fee for the residential programme is approximately ฿280,000 per month (~$8,500 USD).
What that covers and what it does not:
| Included in the fee | Billed separately |
|---|---|
| Private accommodation, all meals, housekeeping | Medication the doctor prescribes (including taper medications and non-opioid pain medications) |
| Group and individual therapy, daily schedule | Flights and visa fees |
| Visiting psychiatrist — intake assessment and routine progress checks | Additional psychiatric consultations beyond the included visits |
| Yoga, fitness sessions, pool access, weekly excursions | Hospital visits and transportation (if needed for severe withdrawal) |
| Two months of structured aftercare | Personal items, additional spa or massage sessions |
For severe opioid withdrawal — typically high-dose long-acting opioids, very high morphine milligram equivalent loads, or significant cardiac or respiratory complications — we may detox you first at our partner hospital, which has intensive and intermediary intensive care units, before you transfer to One Step for the rehab programme. Most prescription-opioid clients do not need this step; the standard residential taper handles them on site. See our treatment programme, treatment schedule, detox approach, and the opioid rehab cluster page for the full clinical picture.
If you have a sibling on the same broader topic, our companion piece on the difference between opiates, opioids and heroin covers the terminology so you can read prescriber notes and pharmacy labels without guessing. For the aftercare side — the long, quieter work that follows the residential stay — see our aftercare programme.
Frequently Asked Questions
Common questions from chronic pain patients considering treatment for prescription-opioid dependence.
Not by the medical definition. Taking opioids exactly as prescribed and developing dependence is a physiological adaptation, not a use disorder. Use disorder requires behavioural features — running out early, taking extra doses, using for mood rather than pain, hiding use — that are absent in compliant patients. Dependence still needs treating if you want off the drug; it just is not the same as addiction.
Slower than you probably want. For someone who has been on opioids for over a year, reductions of 5-10% every one to two weeks are typical, and even slower for higher doses or longer histories. The CDC suggests roughly 10% per month as a safe pace for long-term users. A faster taper triggers withdrawal severe enough that most people return to the drug at their old dose, where tolerance is no longer protective.
Some pain will return, but often less than patients expect — particularly if opioid-induced hyperalgesia has been amplifying it. Many patients report a temporary flare during the taper, then a settling to a lower baseline pain level that is more responsive to non-opioid treatment. Without an alternative pain plan in place, however, the rebound pain is what drives most taper failures, which is why pain management and dependence treatment have to happen together.
Put the request in writing with a specific opening proposal — for example, a 10% reduction over four weeks — so the prescriber has to respond to a defined plan. If they still refuse, ask for a referral to a pain medicine specialist or addiction medicine physician. If neither route works, a residential programme that handles both taper and pain management together is sometimes the most realistic option.
Many patients can taper at home if they have a willing prescriber, a non-opioid pain plan, and a stable household. Residential treatment becomes the right choice when previous home taper attempts have failed, when the chronic pain is severe enough to derail outpatient progress, or when the household environment makes structured recovery hard. Severity of dose is also a factor — high-dose, long-acting opioids are harder to taper outside a clinical setting.
It is a distinct, measurable phenomenon — not the same as rebound pain or tolerance, though they often overlap clinically. Systematic reviews of chronic opioid users have shown experimentally measurable increases in pain sensitivity that go beyond what tolerance alone explains. The practical clue is pain that spreads beyond the original injury or worsens between doses, and that improves rather than worsens as the dose is reduced.
Yes. The residential programme accommodates prescription-opioid clients by pacing the taper individually, coordinating non-opioid pain management with the visiting psychiatrist, and adjusting the therapy work to address the identity strain most of these clients arrive with. For severe withdrawal — high doses or significant medical complications — we may detox you first at our partner hospital, which has intensive and intermediary intensive care units, before you transfer to One Step.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








