Key Takeaways
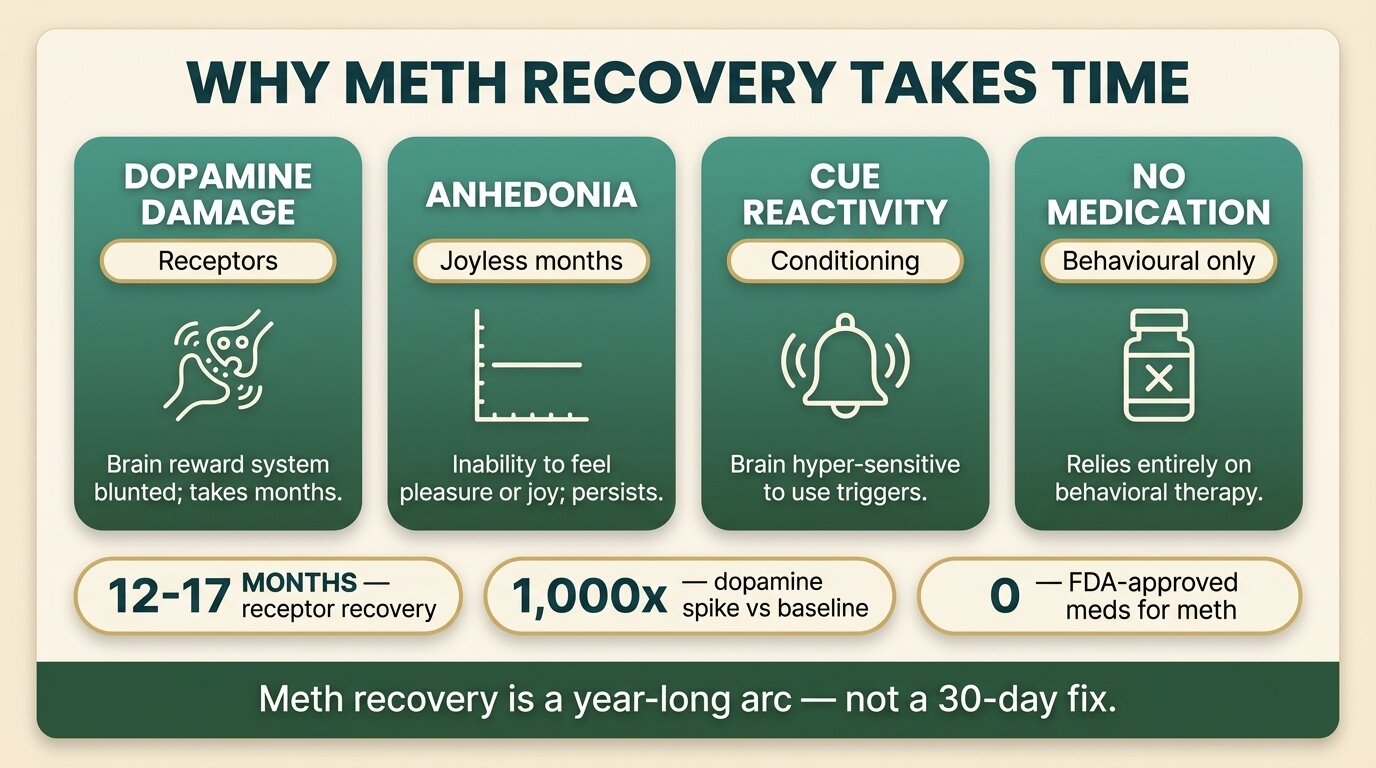
- Meth addiction is hard to quit because it physically downregulates dopamine D2 receptors in the brain — the receptors that let you feel pleasure, motivation, and reward. PET imaging shows partial recovery takes 12–17 months of abstinence, not 30 days.
- The first 1–3 months sober are the “joyless months” — anhedonia, broken sleep, and dysphoria. Most relapses happen here because people interpret the flatness as proof that sobriety doesn’t work.
- There are no FDA-approved medications for methamphetamine use disorder. Unlike alcohol (naltrexone, acamprosate) or opioids (buprenorphine, methadone), the backbone of meth treatment is behavioural — contingency management has the strongest evidence base.
- Cues — places, people, paraphernalia, even certain music — trigger conditioned cravings independent of conscious intent. Returning to the same environment is one of the strongest predictors of relapse.
- What actually works: time, environment change, structure, treating co-occurring conditions, contingency management, and aftercare. Meth recovery is beatable — but the timeline is closer to 12–24 months than 30 days.
Meth addiction is hard to overcome because methamphetamine physically damages the brain’s dopamine system, and that damage takes 12 to 17 months of sustained abstinence to partially repair — not the 30 days most rehab programmes offer. Brain imaging shows that meth users have significantly reduced dopamine D2 receptor availability and dopamine transporter density, which means the brain literally cannot generate normal feelings of pleasure, motivation, or reward during early recovery (Volkow et al., J Neurosci, 2001). If you have tried to quit before and failed, you were not weak. You were fighting neurobiology with willpower, on a clock that ran out months too early.
This post explains the specific reasons meth is so difficult to beat — receptor damage, anhedonia, conditioned cues, the absence of medication options, polysubstance complications, and sleep wreckage — and what the evidence actually shows about getting through them. The honest picture is hard but not hopeless. With enough time, the right environment, and the right structure, the brain does recover. The problem is that almost nobody gives recovery enough time.
Why Does Meth Damage the Dopamine System So Severely?
Meth floods the brain with dopamine at concentrations no natural reward can match — roughly 1,000 times the baseline release. In response, the brain protects itself by downregulating dopamine D2 receptors and reducing dopamine transporter density. After heavy chronic use, these losses are measurable on PET scans and resemble the receptor profile seen in Parkinson’s disease (NIDA, 2024).
This is the single most under-explained piece of meth recovery. When someone says “I just need a few weeks to clear my head,” they are working with a model of addiction that doesn’t apply to meth. The dopamine system has structurally changed. The receptors that let you feel ordinary pleasure — from food, conversation, sex, sunlight — are physically fewer in number, and the cells that recycle dopamine are damaged.
Imaging studies show that partial recovery of dopamine transporter function is possible, but only after 12 to 17 months of continuous abstinence. Even then, striatal metabolism in some regions remains lower than in non-users (Wang et al., Am J Psychiatry, 2004). A 28-day or 60-day stay can stabilise you, change your environment, and start the work — but the underlying neurobiology is not going to be fixed in that window. Treatment that pretends otherwise sets people up to relapse and feel like failures.
| Time abstinent | Dopamine D2 receptors | Dopamine transporter | How it feels |
|---|---|---|---|
| 0–6 months | Markedly reduced | Markedly reduced | Anhedonia, no motivation, sleep disrupted |
| 9–12 months | Partial recovery beginning | Partial recovery | Mood lifts gradually, motivation returns |
| 12–17 months | Substantially recovered in many users | Substantially recovered | Closer to baseline, pleasure capacity restored |
| 17+ months | Near-normal in most | Near-normal in most | Stable, with continuing risk of cue-triggered relapse |

What Are the “Joyless Months” and Why Do Most Relapses Happen Then?
The post-acute window — roughly weeks 2 through 12 — is when most meth relapses happen. The acute withdrawal (sleep, crashing, exhaustion) is mostly over within 7 to 10 days, but what follows is harder to endure: persistent anhedonia, depressed mood, broken sleep, and cravings that don’t fade on schedule. In one study, craving was still elevated 5 weeks after the last use (Zorick et al., Addiction, 2010).
People relapse during this window not because they fail to “want it enough,” but because nothing feels good. Food is bland. Sex is uninteresting. Music is flat. The reward system that used to make ordinary life worth getting up for is — temporarily — offline. Without explanation, this period reads as proof that sobriety is empty. With explanation, it reads as a known stage of healing that will pass.
Acute withdrawal studies confirm anhedonia, irritability, and poor concentration as the dominant symptoms of early abstinence (Newton et al., Am J Addict, 2004). McGregor and colleagues mapped the timeline more precisely: an acute phase of 7–10 days with high-intensity symptoms, followed by a subacute phase of at least two more weeks of lower-grade but persistent depression and craving (McGregor et al., Addiction, 2005). What both studies miss, and what longer-arc imaging studies fill in, is that the subacute symptoms — particularly the mood and motivation deficits — can persist for months in heavier users.
This is why duration of treatment matters more than intensity for meth recovery. A reader who is on day 35 of sobriety and feels nothing is not failing. They are at a predictable, neurobiological midpoint. Treatment that includes CBT and DBT, structured days, and physical activity can help bridge this window, but the window itself has to be crossed — there is no shortcut around it.
How Do Conditioned Cues Trigger Cravings Even When You Don’t Want to Use?
Cue reactivity is the technical name for what most meth users have experienced and many find shameful: walking past a certain street, hearing a certain song, or seeing a glass pipe in a film triggers a wave of craving you didn’t choose. fMRI studies show that meth-related cues activate the ventral striatum, caudate, and medial prefrontal cortex — the same circuitry that drives reward-seeking. This is Pavlovian conditioning, not weakness (Seow et al., Int J Environ Res Public Health, 2020).
Years of pairing the drug with specific environments, people, paraphernalia, and times of day creates automatic learning the brain cannot simply switch off. The strongest predictor that an early-recovery person will relapse is returning to the same physical and social environment in which they used. This is one of the strongest arguments for residential treatment away from your home city: removing the cues for long enough to weaken the pairing.
For a fuller breakdown of the cue categories meth users face, see our guide to the 10 most common relapse triggers and how to plan for each. The patterns that matter most for meth recovery: paraphernalia, certain types of sexual activity (chemsex is a major and under-discussed trigger), specific music, certain hours of the night, and any person you used with regularly.
The mistake I see most often is people interpreting receptor recovery time as a moral failure. They quit, feel nothing for three months, decide it isn’t working, and use again. What they are describing is the neurobiology working exactly as the imaging studies predict. The receptors are not back yet. That is not a sign you’ve failed — it’s a sign you need to stay the course longer, in an environment that supports it.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab

Why Are There No FDA-Approved Medications for Meth Addiction?
There are no FDA-approved medications for methamphetamine use disorder. Alcohol has naltrexone, acamprosate, and disulfiram. Opioids have buprenorphine, methadone, and naltrexone. Nicotine has varenicline and patches. Meth has none (NIDA, 2024). The reasons are scientific, not political: meth’s mechanism — flooding presynaptic dopamine release — has resisted every receptor-blocker, agonist, and replacement strategy researchers have tried.
Trials have looked at mirtazapine, bupropion, naltrexone, varenicline, modafinil, and topiramate. Some show modest signals in specific subpopulations. None has hit the bar for FDA approval. The most promising recent work is the ADAPT-2 trial of injectable naltrexone plus extended-release bupropion, but even that combination is not approved for meth treatment as of 2026.
| Substance | FDA-approved medications | Mechanism that makes treatment possible |
|---|---|---|
| Alcohol | Naltrexone, acamprosate, disulfiram | Targets reward pathway and aversive conditioning |
| Opioids | Buprenorphine, methadone, naltrexone | Receptor agonist/antagonist substitution |
| Nicotine | Varenicline, NRT, bupropion | Partial agonist at nicotinic receptors |
| Methamphetamine | None | Floods dopamine release — no clean receptor target |
This absence is why supportive care — therapy, structured environment, contingency management, treatment of co-occurring conditions, and time — is the entire backbone of meth treatment. Some clients at our facility are prescribed off-label medication for sleep, mood, or anxiety during their stay; medication is billed separately and depends on the doctor’s assessment.
The strongest-evidenced behavioural treatment is contingency management — small tangible rewards (cash, vouchers, prizes) for negative urine drug screens and treatment milestones. More than 100 trials support it; NIDA and SAMHSA both list it as the best-evidenced approach for stimulant use disorder (SAMHSA TIP 33, 2021). It is not yet widely available outside the United States, but the underlying principle — frequent, structured, positive reinforcement for visible recovery behaviour — is something a good treatment programme can replicate in other forms.
Tried to quit before and feel like you failed? Talk to our team — we’ll give you a straight answer about whether longer-stay residential treatment in Chiang Mai makes sense for your situation.
Why Does Polysubstance Use Make Meth Recovery Even Harder?
Most heavy meth users are not single-substance users. Many use alcohol to come down, ketamine or GHB to sleep, opioids to manage agitation, or other stimulants between sessions. Quitting meth while continuing to drink heavily or use other depressants is one of the most common relapse pathways — the other substance keeps the reward circuitry primed and provides a stepping-stone back to meth.
This matters clinically because true meth recovery means addressing the full substance pattern, not just the headline drug. A reader who stops meth but continues drinking a bottle of whisky a night is not in recovery; they are managing one substance with another. Treatment that doesn’t ask about and treat the secondary substances will fail at the first stressor.
Chemsex — the use of meth, often with GHB, ketamine, or mephedrone, during sexual activity — is a particularly hard pattern to break because the meth craving is fused with sexual cues. The two reinforce each other in the same conditioned learning that drives cue reactivity. Posts about meth recovery that don’t acknowledge chemsex are missing the cohort most at risk.
How Long Does Sleep Take to Recover After Meth?
Meth blows up sleep architecture in ways that take months to repair. Polysomnography studies of meth users in early remission show reduced sleep efficiency, prolonged REM latency, and altered non-REM sleep stages even at three months sober — well beyond the typical “withdrawal” window most rehabs plan for (Rezaei-Ardani et al., Sleep Sci, 2021). Broken sleep is not a minor inconvenience — it is one of the strongest predictors of relapse.
Why sleep matters so much: sleep is when the brain consolidates new learning, including the new behavioural patterns recovery requires. Sleep deprivation impairs impulse control, amplifies cravings, worsens depression, and degrades the prefrontal-cortex regulation people need to refuse a cue-triggered urge. A meth user trying to recover on four broken hours of sleep a night is fighting with both hands tied.
What actually helps: rigid wake-and-sleep times (the same time every day, including weekends), morning daylight exposure, physical activity during the day, no screens in the hour before bed, and — under medical supervision — short courses of non-addictive sleep medication during the worst weeks. Caffeine and nicotine matter more than people think; cutting both substantially in the first 90 days speeds sleep recovery.
What Does the One Step Approach to Meth Recovery Look Like?
One Step gives meth clients the one thing the neurobiology actually requires: time and structure in an environment where the cues are gone. We run residential treatment in Chiang Mai, typically 28 to 90 days, with most meth clients staying closer to the upper end of that range. The base programme fee is approximately ฿280,000/month (about $8,500 USD); medication, flights, visas, and personal items are billed separately.
The treatment programme combines individual counselling, group therapy, CBT and DBT, physical activity, and a fixed daily structure. Days start early. Meals, therapy, and exercise sit at the same times each day. Phones are restricted in the first phase. The point of all of this is not to be punishing — it is to install a rhythm the dopamine-depleted brain can follow when its own motivation is offline.
For people coming off heavy meth use, on-site detox is generally straightforward — meth withdrawal is not medically dangerous in the way severe alcohol or benzodiazepine withdrawal can be. We can handle it residentially. What it requires is supervision, sleep support, and patience through the first 10 days. For an honest day-by-day breakdown, see our guide to how long meth detox takes.
If you’re trying to understand the differences between meth, amphetamine, and crystal meth in particular — and how those differences shape both the addiction pattern and the recovery arc — read our meth rehab overview and our explainer on methamphetamine vs amphetamine vs crystal meth.
We are honest with prospective clients about timelines. A 28-day stay can stabilise you and start the work. A 60- to 90-day stay does substantially more. The neurobiology of meth recovery does not finish in a residential programme — it finishes in the year of aftercare that follows. We build the second half of that arc into the conversation from intake.

What Actually Works for Meth Recovery?
Meth recovery works when you stack the things the evidence supports — time, environment, structure, treatment of co-occurring conditions, contingency-management-style reinforcement, and a long aftercare arc. No single intervention does the job; the stack does. Each element compensates for the absence of an FDA-approved medication and for the long timeline of receptor recovery.
| Element | Why it matters | What “doing it” looks like |
|---|---|---|
| Time | Dopamine receptors recover over 12–17 months | Plan in months and years, not days and weeks |
| Environment change | Removes conditioned cues | Residential treatment away from use environment |
| Daily structure | Fills the vacuum a meth-organised life leaves behind | Fixed wake, meal, therapy, exercise times |
| Co-occurring care | Untreated depression, ADHD, trauma drive relapse | Psychiatric assessment + targeted treatment |
| Reinforcement | Contingency management has the strongest evidence base | Structured rewards for visible recovery milestones |
| Aftercare | Receptor recovery isn’t done at discharge | 12+ months of community, sponsor, or therapist contact |
The single piece readers should not skip: plan for a year, not a month. Most people who succeed at meth recovery measure their first year in 12 thirty-day blocks, not in a single 30-day window followed by “back to normal life.” The brain is on a 12-to-17-month timeline whether your calendar is or not.
If you or someone you love is struggling with substance dependence, explore how a professional drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions from people facing meth addiction or supporting someone who is.
Acute withdrawal resolves in 7–10 days, but PET imaging shows the dopamine system takes 12 to 17 months of continuous abstinence to partially recover. Plan for a one- to two-year arc, not a 30-day fix. A residential programme is the starting point, not the finish.
Meth withdrawal is not medically dangerous in the way severe alcohol or benzodiazepine withdrawal can be. It is, however, psychologically brutal — heavy fatigue, depression, anhedonia, and intense cravings. Most clients can detox from meth in a residential setting with appropriate supervision and sleep support.
No. There are no FDA-approved medications for methamphetamine use disorder. Some off-label medications can help with sleep, mood, or co-occurring conditions during recovery, but the backbone of treatment is behavioural — therapy, structured environment, and contingency management have the strongest evidence base.
This is called anhedonia and it is a normal stage of meth recovery, not a sign sobriety has failed. Dopamine D2 receptors are still downregulated, which means ordinary pleasure cannot register the way it used to. For most people the flatness starts to lift between months 3 and 9, and continues improving through month 12 and beyond.
Substantially yes, in most users. Brain imaging shows dopamine transporter density and metabolism in most brain regions recover to near-normal after 12 to 17 months of continuous abstinence. Some studies suggest small residual differences in specific striatal regions, but functionally most people regain normal mood, motivation, and pleasure capacity.
That is cue reactivity — Pavlovian conditioning that pairs the drug with environments, objects, people, and sensory cues over years of use. fMRI shows these cues activate the same reward circuitry meth itself activates. The good news is that with repeated cue exposure without use, the pairing weakens. The cravings get shorter and less intense over time.
Meth produces dopamine release roughly 1,000 times above baseline — orders of magnitude more than alcohol, cannabis, or even cocaine. The neurobiological hole that leaves behind is correspondingly larger, and the recovery timeline is correspondingly longer. Quitting meth is harder for measurable, structural reasons, not because of any deficiency in you.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn