
Key Takeaways
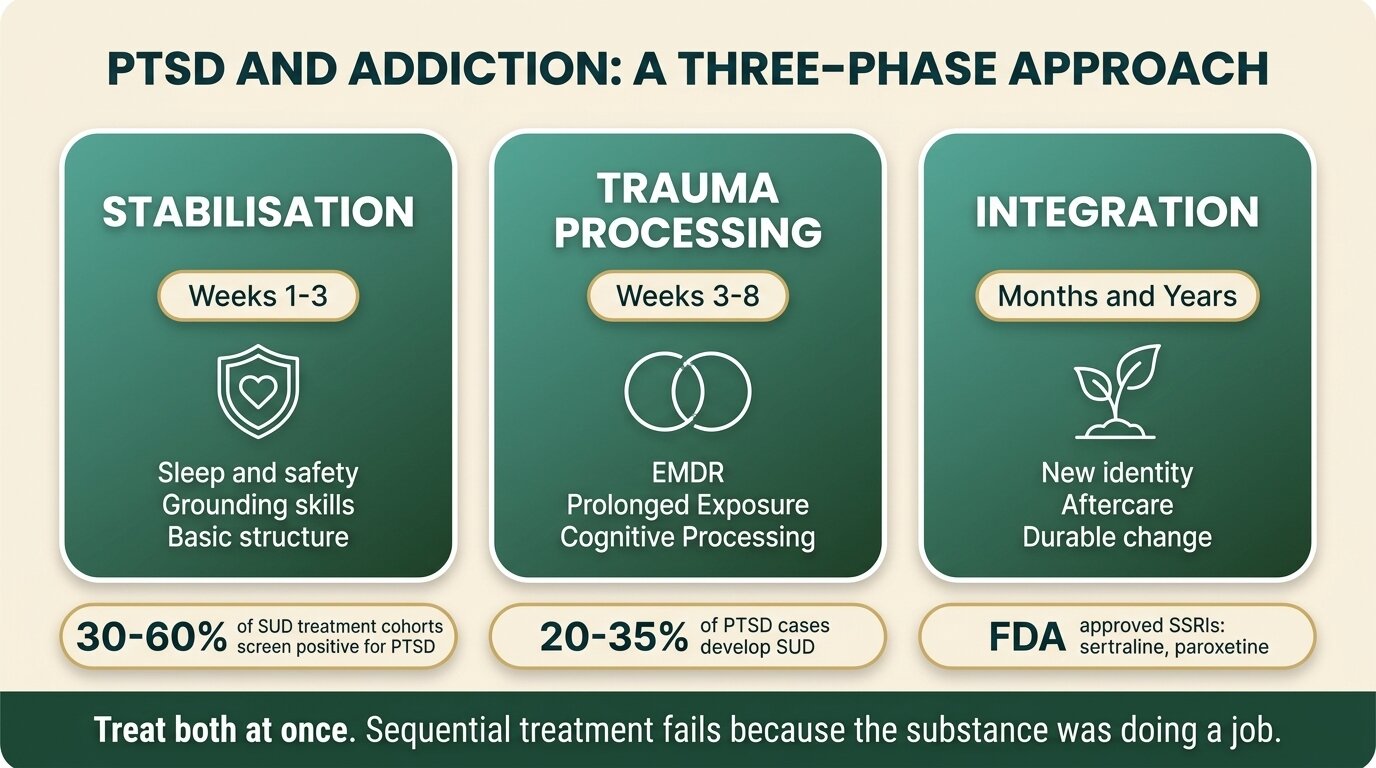
- Roughly 30-60% of people in substance use treatment screen positive for trauma, and an estimated 20-35% of people with PTSD develop a substance use disorder. The two conditions are linked, not coincidental.
- The substance was doing a job. Alcohol, cannabis and benzodiazepines blunt hypervigilance and nightmares. Opioids dull emotional pain. Stimulants pull people out of depressive collapse. That is why “just stop drinking” almost never works on its own.
- Sequential treatment (“get sober first, then deal with the trauma”) fails predictably. When the substance comes off, PTSD symptoms intensify — and without trauma treatment running in parallel, relapse is the most likely outcome.
- Integrated treatment is the evidence-based standard. The 2023 VA/DoD guideline confirms that trauma-focused therapies — EMDR, Prolonged Exposure (PE), Cognitive Processing Therapy (CPT) — can be safely delivered alongside substance use treatment, and that having an SUD should not delay PTSD care.
- Benzodiazepines are usually the wrong answer. Research links them to worse PTSD outcomes, increased aggression, depression and substance misuse. SSRIs (sertraline, paroxetine) and prazosin for nightmares have stronger evidence.
If your drinking, cannabis, opioid or stimulant use started — or got much worse — after a trauma, you are not weak and you are not “just” an addict. You are doing what an estimated 30-60% of people in addiction treatment do: using a substance to quiet a nervous system that has not felt safe since something happened to you (Hawn et al., J Trauma Stress, 2020). This article is about why that pattern develops, why sequential “sober first” treatment so often fails, and what an integrated approach to PTSD and addiction actually looks like.
It is also about what trauma-informed treatment is not. It is not a tidy narrative — find your trauma, process it, finish. Recovery from PTSD and addiction together is rarely linear, and any programme that promises otherwise is selling you something.
How Often Do PTSD and Addiction Occur Together?
Estimates vary by setting, but the overlap is well-established: roughly 20-35% of people with PTSD develop a substance use disorder, and 25-50% of people in active SUD treatment meet criteria for current PTSD, with lifetime rates closer to 30-40% on average (NIDA, 2024). Among combat veterans, women, and survivors of childhood abuse, the rates are higher still.
The pattern shows up in specific populations: combat veterans (especially those with multiple deployments), survivors of sexual assault, first responders, survivors of intimate partner violence, and adults carrying high adverse childhood experience (ACE) scores. In adolescent and young adult justice-involved samples, more than 70% meet criteria for an SUD and around half meet criteria for PTSD — rates dramatically higher than community samples.
The clinical implication is simple. If you arrived at a substance use problem and a trauma history brought you there, you are not an unusual case. You are the common case. The unusual case is the person whose substance use has no trauma underneath it at all.
| Population | PTSD rate | SUD rate | Source pattern |
|---|---|---|---|
| General US adults (lifetime) | ~6.8% | ~8.4% | National epidemiology |
| People with PTSD | 100% (definitional) | 20-35% comorbid SUD | NCS, NESARC data |
| People in SUD treatment | 25-50% current PTSD | 100% (definitional) | Treatment cohorts |
| Combat veterans (post-deployment) | 10-30% | 30-60% in PTSD+ vets | VA data |
| Justice-involved young adults | ~50% | ~70% | Forensic cohorts |

Why Do People With PTSD Use Substances?
The dominant explanation is the self-medication hypothesis — first formulated by Edward Khantzian in the 1970s and 80s — which proposes that people with psychiatric symptoms gravitate toward substances that specifically blunt those symptoms (Khantzian, Harv Rev Psychiatry, 1997). In PTSD, each symptom cluster has a substance that tends to mute it.
That is why most people with PTSD have a clear primary drug of choice. It is not random. It is doing a specific job — and the job is usually to make the inside of the head quieter so that sleep, work, sex, parenting, or simply existing in a room becomes possible again.
| PTSD symptom cluster | What it feels like | Substance often used to blunt it |
|---|---|---|
| Hyperarousal / hypervigilance | Constant scanning, startle, racing heart, can’t relax in a room | Alcohol, cannabis, benzodiazepines |
| Intrusions / nightmares / flashbacks | Replay loops, sweats, terror sleep, sudden re-experiencing | Alcohol, cannabis, benzodiazepines (for sleep) |
| Emotional pain / shame / grief | A specific ache that won’t dissolve; physical heaviness in the chest | Opioids |
| Numbing / depressive collapse | Flat, detached, can’t get out of bed, nothing matters | Cocaine, methamphetamine, other stimulants |
| Dissociation | Foggy, unreal, watching yourself from outside, time slipping | Cannabis, ketamine, alcohol (mixed pattern) |
The framework is not perfect — research on PTSD with comorbid alcohol use offers strong but not universal support, and people often shift substances as PTSD evolves (Hawn et al., J Trauma Stress, 2020). But the clinical pattern shows up reliably enough that “what does this person’s substance actually do for them?” is one of the most useful questions to ask at intake.
Why Does “Get Sober First, Then Deal With the Trauma” Fail?
Sequential treatment fails for a mechanical reason: the substance was holding the trauma symptoms down. Take the substance off and the symptoms come back louder than before, because the nervous system has lost both its symptoms and its main coping tool in the same week. Without trauma treatment running alongside the abstinence work, relapse is the predictable outcome.
This is not a moral failing or a willpower problem. Anyone with a working understanding of PTSD physiology can see why it happens. Trauma rewires the threat-detection system to stay switched on. Alcohol, benzodiazepines and cannabis blunt that system pharmacologically. Detox removes the blunt and the threat-detection system rebounds — often above pre-substance baseline. Sleep collapses. Nightmares return. Hypervigilance becomes unbearable. The person discovers that they were not, in fact, “just” an addict; the substance was doing something specific that nothing else was doing.
For decades the field treated this as a problem to solve sequentially — stabilise the addiction, then refer out for trauma treatment. The evidence has shifted. The 2023 VA/DoD Clinical Practice Guideline for PTSD now states that having a substance use disorder should not prevent or delay evidence-based PTSD treatment, and that integrated, trauma-focused interventions show the largest benefit relative to single-disorder approaches (VA National Center for PTSD, 2023).
This is also why we link this article to our work on dual diagnosis treatment and on the types of dual diagnosis therapies we use. The mental health condition and the substance use disorder are not two problems in a queue. They are one problem with two faces.

What Does Integrated PTSD and Addiction Treatment Actually Look Like?
An integrated approach treats PTSD and the substance use disorder in the same clinical setting, by the same team, in the same week — not as two separate referrals. In practice it runs in three loose phases: stabilisation (safety, sleep, basic skills), trauma processing (EMDR, PE, CPT or TF-CBT once stable), and integration (rebuilding identity beyond “the trauma” and “the addict”). The phases overlap and people loop back through them; recovery is not linear.
Phase 1: Stabilisation
You cannot do trauma processing on a nervous system that is in active withdrawal or in physical danger. Phase 1 is about getting sleep back, getting the body fed and rested, learning grounding and breathing skills, and building enough safety in the daily structure that the rest of the work becomes possible. For most people this takes the first 1-3 weeks of a residential stay.
Phase 2: Trauma processing
Once stabilised, the actual trauma work begins. Several therapies have strong evidence:
- EMDR (Eye Movement Desensitization and Reprocessing) — bilateral stimulation while recalling the trauma; one of the three trauma-focused therapies the VA/DoD guideline strongly recommends. We cover the mechanism in detail in EMDR for Trauma and Addiction.
- Prolonged Exposure (PE) — repeated, structured retelling of the trauma memory in a safe setting, plus graded real-world exposure.
- Cognitive Processing Therapy (CPT) — identifies “stuck points” in how the trauma is being interpreted (often around guilt, blame, or self-worth) and works on rewriting them.
- Trauma-Focused CBT (TF-CBT) — combines exposure with cognitive restructuring; widely used with younger adults and adolescents.
- Seeking Safety — Lisa Najavits’ manualised, present-focused model designed specifically for PTSD+SUD; emphasises safe coping skills rather than trauma processing, useful in early stabilisation or where trauma-focused work is not yet tolerable (Najavits et al., J Trauma Stress, 1998).
The largest multi-site trial of Seeking Safety, conducted within NIDA’s Clinical Trials Network with 353 women in SUD treatment with co-occurring PTSD, found significant PTSD symptom reductions across both Seeking Safety and an active control, with high treatment alliance ratings for Seeking Safety in particular (Hien et al., Am J Psychiatry, 2009). Subsequent guidance from the VA notes that present-focused coping models like Seeking Safety are generally less effective for PTSD symptom reduction than trauma-focused therapies, but remain valuable for stabilisation and engagement.
Phase 3: Integration
The third phase is the one most rehab programmes skip. After the trauma loses its grip and abstinence is established, the person still has to rebuild an identity that is not organised around being “the trauma survivor” or “the addict.” This is what aftercare, peer support, and ongoing therapy are actually for — and why we put so much weight on structured aftercare after discharge.
The mistake we still see referred from other programmes is treating the substance and the trauma as a queue. Detox, then maybe refer for trauma later. By the time “later” arrives the person has relapsed twice. When PTSD is driving the use, you have to treat both in the same room, in the same week. The substance was not the problem. It was the answer to a problem nobody had treated.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
If trauma is driving the drinking or using, you need a programme that treats both. Talk to our team — we will tell you honestly whether we are the right fit for your situation.
What Medications Help PTSD, and Which Ones Make It Worse?
Medication for PTSD is supportive, not curative — it makes therapy possible by lowering the volume on hyperarousal, intrusions and nightmares. The two SSRIs with FDA approval for PTSD are sertraline (Zoloft) and paroxetine (Paxil); venlafaxine (an SNRI) is also recommended first-line by the 2023 VA/DoD guideline. Prazosin has specific evidence for trauma-related nightmares. Benzodiazepines are usually the wrong answer and have evidence of harm in PTSD populations.
| Medication | What it targets | Evidence | Notes in SUD |
|---|---|---|---|
| Sertraline (Zoloft) | Overall PTSD symptoms, mood | FDA approved for PTSD; first-line | Safe in active SUD; 6-12+ months |
| Paroxetine (Paxil) | Overall PTSD symptoms, mood | FDA approved for PTSD; first-line | Safe in active SUD; discontinuation symptoms if stopped abruptly |
| Venlafaxine (Effexor) | Overall PTSD symptoms | First-line per 2023 VA/DoD | BP monitoring at higher doses |
| Prazosin | Trauma-related nightmares, sleep | Mixed; recommended for nightmares in 2023 VA/DoD | Useful add-on when nightmares are dominant |
| Benzodiazepines | Anxiety, sleep (short-term) | No PTSD benefit; associated with worse outcomes | Relatively contraindicated in PTSD and SUD |
The 2015 systematic review by Guina and colleagues, looking at 18 trials and observational studies, concluded that benzodiazepines are ineffective for PTSD treatment and prevention, and that “risks associated with their use tend to outweigh potential short-term benefits” — including increased likelihood of developing PTSD after recent trauma, diminished therapy effectiveness, and elevated rates of aggression, depression and substance misuse (Guina et al., J Psychiatr Pract, 2015). In a population that already has a substance use disorder, the calculation is even clearer.
This is the awkward conversation we sometimes have with clients who arrive on a long-term benzodiazepine prescription written for “PTSD anxiety.” The medication may be doing something in the short term, but the evidence does not support it as a PTSD treatment, and tapering is usually part of the plan — done slowly and medically, never abruptly.
How Does One Step Treat PTSD and Addiction Together?
We treat PTSD and substance use in the same residential programme rather than referring trauma work out. Our visiting psychiatrist handles SSRI and other medication decisions, our therapists include EMDR-trained practitioners, and the daily structure is built to support trauma-informed care: predictable rhythm, set wake times, group work where appropriate, individual work where group is too much. We are not a specialist combat-veteran unit and we are not a locked psychiatric facility — we are a residential rehab programme that takes the trauma part seriously instead of treating it as someone else’s job.
The fee is approximately ฿280,000/month (~$8,500 USD). That covers accommodation, therapy hours, group work, intake and routine progress checks with the visiting psychiatrist, and the standard daily programme. Medication is billed separately — you pay for what the doctor prescribes, including SSRIs, prazosin or any taper protocol. Flights, visas, additional one-to-one counselling, hospital visits and personal items are also not included. See our full pricing page and treatment programme for the detail.
On scope: we run trauma-informed care within a residential addiction programme. That works well for most people whose PTSD and substance use have been driving each other, including survivors of violent relationships, sexual assault survivors, first responders, and adults with high ACE scores. It is not the right setting for someone in acute psychiatric crisis requiring inpatient psychiatric hospitalisation, or for severe complex C-PTSD with severe dissociation that needs a longer phased trauma stabilisation than residential rehab can offer. For those cases we will say so at assessment and help direct you to a setting that fits.
Most clients stay 28-60 days. PTSD work in particular benefits from longer stays — the stabilisation phase alone can take 2-3 weeks before trauma processing becomes possible. We will tell you that upfront rather than book you for a fortnight and pretend the trauma will resolve in time.
What Should Recovery From PTSD and Addiction Actually Look Like?
Non-linear, and slower than the marketing of any rehab suggests. Recovery from PTSD and SUD together usually involves stabilisation, trauma processing, slips and returns, identity rebuilding, and ongoing aftercare over years — not a 28-day arc with a finish line. Programmes that promise a tidy resolution are misreading both conditions. The realistic frame is durable management, not a cure.
Some practical implications. Expect setbacks; they are data, not failure. Expect that some sessions will feel useless and others will move years of stuck material in 90 minutes. Expect that an aftercare plan with a clear map of your relapse triggers matters more than any brochure promise of permanent fix. And expect that the work of building an identity beyond the trauma — the third phase — is often the longest, even though it gets the least airtime.
Frequently Asked Questions
Common questions about PTSD, addiction, and integrated treatment.
The 2023 VA/DoD guideline says that having an active substance use disorder should not prevent you from receiving evidence-based PTSD treatment. Trauma-focused therapies like EMDR, Prolonged Exposure and Cognitive Processing Therapy can be delivered safely alongside substance use treatment in an integrated programme. In a residential setting, stabilisation typically comes first, then trauma processing once sleep and safety are in place.
Yes, in the right phase. EMDR is one of the three trauma-focused therapies the VA/DoD guideline recommends, and it can be delivered to people with co-occurring SUD. It is usually not started during active withdrawal or before the person has basic grounding skills and stable sleep. Once stabilised, EMDR can move material that talk therapy alone has not shifted.
The systematic review evidence shows benzodiazepines do not improve PTSD symptoms and are associated with worse outcomes — including increased aggression, depression, substance misuse, and reduced effectiveness of trauma-focused therapy. In someone who already has an SUD, the addiction risk compounds the problem. SSRIs (sertraline, paroxetine), venlafaxine and prazosin for nightmares have stronger evidence and are preferred.
Some trauma-focused therapies (Prolonged Exposure, CPT) involve structured retelling of the event. EMDR involves bringing the memory to mind but does not require detailed verbal narration. Present-focused models like Seeking Safety do not require trauma processing at all and focus on coping skills. A good integrated programme matches the approach to where you are, not the other way round.
Residential treatment is usually 28-60 days for the intensive phase, with the stabilisation phase taking 1-3 weeks before trauma processing begins. The full recovery — including identity rebuilding and durable change — is measured in years, not weeks. Aftercare and continued therapy are part of the plan, not an optional extra.
The clinical threshold for PTSD requires exposure to a qualifying event plus specific symptom clusters. But sub-threshold trauma symptoms — without the full PTSD diagnosis — still respond to trauma-informed treatment and still drive substance use in many cases. A proper assessment will look at the symptoms, not just whether the event “qualifies.” If trauma is driving the using, it is worth treating regardless of the formal label.
We treat veterans and first responders within our standard integrated PTSD and addiction programme. We are not a specialist combat-veteran unit — if you need a service organised entirely around veteran identity and culture, a dedicated veterans programme may be a better fit. For most veterans and first responders whose PTSD and substance use are driving each other, an integrated trauma-informed residential setting works well.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








