Key Takeaways
- Treatment dose matters most. NIDA says fewer than 90 days of treatment is of limited effectiveness — residential delivers that dose; outpatient rarely does in real life.
- Completion rates roughly double in residential settings. A 2016 analysis of U.S. treatment data found residential completion at 65% versus 52% outpatient, and after controlling for confounders, residential clients were nearly three times more likely to finish.
- Environmental reset is the under-rated benefit. Removing the dealer, the drinking partner, the trigger street, and the bottle in the cupboard is something no outpatient program can replicate.
- Integrated care under one roof. Mild-to-moderate detox, daily therapy, medication management, and structured peer support happen in the same building, with the same team, in the same week.
- Outpatient is not bad — it’s just different. It works for people with stable housing, an intact support system, and a manageable addiction. For everyone else, residential gets you over the line.
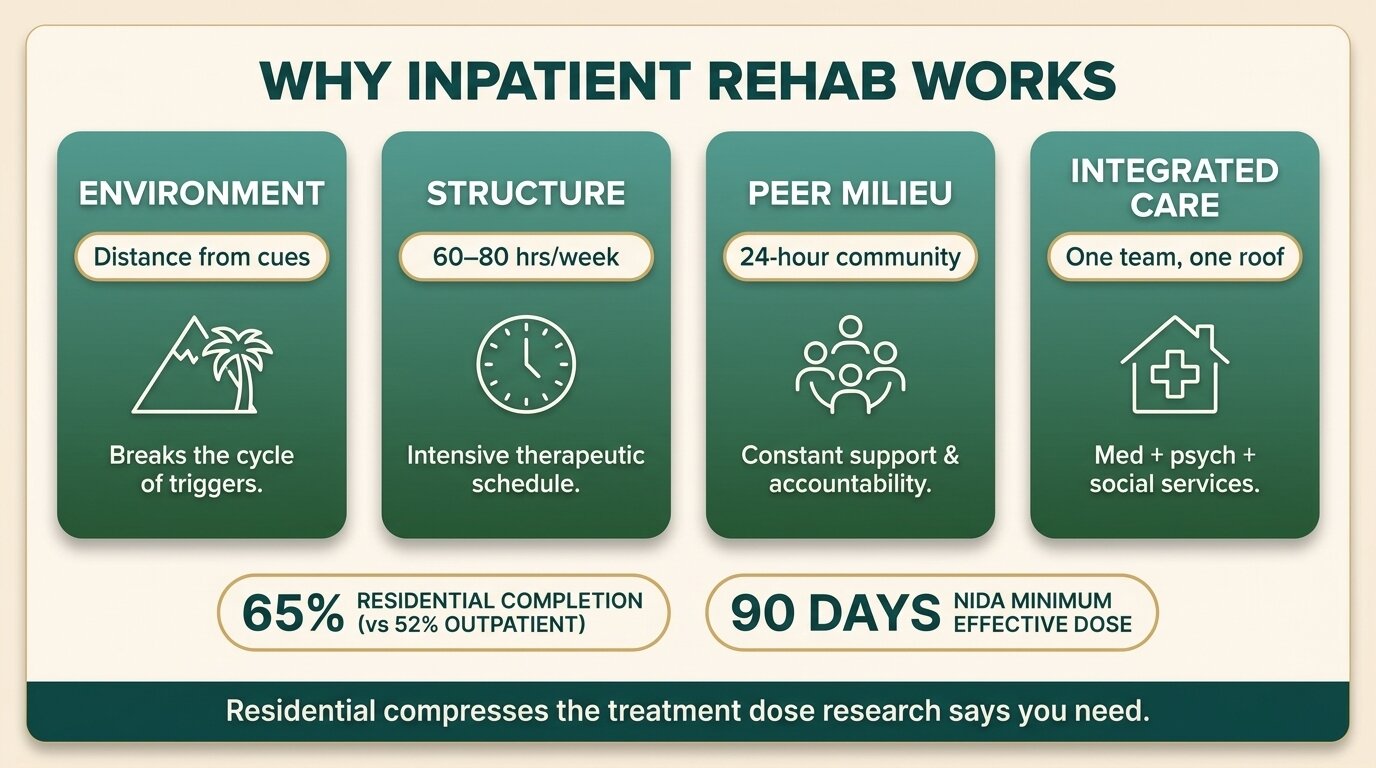
Inpatient substance abuse rehab works because it changes three things at once: your environment, your daily structure, and the people around you — all while delivering the treatment dose research says you actually need. A 2016 analysis of U.S. treatment data found residential clients were nearly three times more likely to complete treatment than outpatient clients after adjusting for severity (Stahler et al., Addictive Behaviors, 2016). The U.S. National Institute on Drug Abuse states bluntly that participation under 90 days is of limited effectiveness (NIDA, 2018). Residential rehab makes that dose realistic. This is the evidence-led case for going inpatient — including the honest trade-offs.
What Does Inpatient Rehab Actually Add That Outpatient Can’t?
Inpatient rehab adds four things outpatient cannot reliably deliver: physical distance from people, places, and substances that cue use; a fully structured 16-hour day instead of 3–9 hours of therapy a week; an immersive peer milieu of people in the same fight; and integrated medical, therapeutic, and pharmacological care happening under one roof with one team.
Outpatient asks you to do hard recovery work while still going home to the environment that built the addiction. That works for some people. It doesn’t work for most. A systematic review of residential treatment studies between 2013 and 2018 found moderate-quality evidence that residential treatment reduces substance use and improves mental health, with positive effects also seen on crime and social outcomes (de Andrade et al., Drug and Alcohol Dependence, 2019).
The four mechanisms below are how residential earns those outcomes.

Why Does the Environmental Reset Matter So Much?
Environment is one of the strongest predictors of relapse. The bottle in the kitchen cupboard, the dealer’s number in your phone, the bar on the corner, the colleague who drinks with you — these are conditioned cues that trigger craving automatically. Inpatient rehab physically removes you from all of them for 28 to 90 days, giving your brain time to weaken those associations before you have to face them again.
This isn’t a soft benefit. The conditioned-cue response is one of the most-studied mechanisms in addiction neuroscience, and it’s one of the reasons relapse rates are so high in the first 90 days post-detox. NIDA lists it as a core principle: effective treatment must address the environmental factors that drive use, not just the substance itself (NIDA, 2018).
At One Step, the reset is geographic as well. We’re in Chiang Mai — different country, different climate, different food, different language. For clients coming from the UK, Australia, or the U.S., that distance is part of the treatment. You can’t walk to the off-licence at 9pm because there isn’t one in the same way, and the friend who’d usually message you at 6pm is asleep.

How Does a Structured Day Make a Difference?
A structured day removes the moment-to-moment decisions that addiction exploits. Wake time, breakfast, therapy, group, exercise, lunch, more therapy, free time, dinner, evening meeting, lights out — every block is pre-decided. You don’t have to summon willpower to skip the 3pm drink because at 3pm you’re in group therapy, not at home wondering what to do.
Outpatient programmes typically deliver 3 to 9 hours of structured care per week. Inpatient delivers 60 to 80. That’s not a marginal difference; it’s an order of magnitude. And those hours include the unstructured time addiction usually fills — evenings, weekends, the gap between work and bed.
The 2019 CADTH review of residential treatment found that residential care was at least as effective, and in many comparisons more effective, than less-intensive treatment options across the included studies (CADTH, 2019). Structure is part of why.

What Is the Peer Milieu and Why Does It Work?
The peer milieu is the community of clients living and treating together. You eat with people in withdrawal, run with people six weeks ahead of you in the programme, and listen to someone in group therapy describe the exact thought pattern you had two days ago. That shared experience does something one-on-one outpatient cannot replicate: it normalises recovery and de-shames addiction.
Group therapy is the workhorse of residential treatment for a reason. Hearing your story in someone else’s mouth interrupts the isolation that fuels relapse. It also builds accountability — you can lie to a therapist for an hour a week. You can’t lie to twelve people you live with for sixty days.
For our clients with co-occurring depression, anxiety, or trauma, this milieu is often the first time they’ve been in a room of people who actually understand. That experience is part of why integrated dual diagnosis care works better in residential settings than as bolt-on outpatient sessions — see our guide to personalised dual diagnosis therapy options and the types of dual diagnosis therapies we use on the programme.
How Does Integrated Detox, Therapy and Medication Work Under One Roof?
Integrated care means medical detox, psychotherapy, psychiatric medication management, and aftercare planning all happen with the same team, in the same place, in the same week. There’s no referral letter, no gap between detox and therapy, no waiting list. A symptom that emerges in detox at 11pm informs the therapist’s plan at 9am the next morning.
Fragmented care is one of the biggest predictors of dropout. In an outpatient model, you detox at one facility, see your therapist at another, get medication from a GP who doesn’t know you, and try to attend mutual support meetings on top of full-time life. Each handoff is a place to fall through the cracks. Residential closes those gaps.
For most substances — cocaine, methamphetamine, ketamine, cannabis, mild-to-moderate alcohol use — One Step handles detox on-site as part of the programme, with our visiting psychiatrist available for assessment and medication. For severe alcohol, benzodiazepine, or opioid dependence requiring ICU-level monitoring, we detox you first at our partner hospital — which has intensive and intermediary intensive care units — then you transfer to One Step for the rehab programme. Either way, the rehab is one continuous process, not three separate ones. More on the medical side in our guide to addiction detox in Thailand.
Why Does Treatment Length Matter More Than Facility Type?
NIDA’s research base is clear: remaining in treatment for an adequate period is critical, and fewer than 90 days yields limited effectiveness for most substance use disorders. Residential makes that 90-day dose achievable. Outpatient asks you to maintain a full year of weekly attendance — possible for some, but the dropout rate is the reason completion is the single biggest predictor of long-term outcome.
The threshold of significant improvement is reached at about three months of continuous treatment, and additional time beyond that adds further gains (NIDA, 2018). Continuing care after the residential stay — what McKay’s review of 20 comparative trials identified as the strongest determinant of post-rehab outcomes — extends that gain over years (McKay, Evaluation Review, 2001; updated narrative review 2009).
This is why our standard recommendation is a minimum 28-day stay, with most clients staying 60 to 90 days. Anything shorter rarely produces lasting change. See who qualifies for inpatient alcohol rehab for the criteria we use at intake.
| Factor | Inpatient / Residential | Outpatient |
|---|---|---|
| Structured care per week | 60–80 hours | 3–9 hours (IOP: 9–12) |
| Typical length | 28–90 days continuous | 3–12 months part-time |
| Environmental separation | Full — different city or country | None — you go home each night |
| Detox handling | On-site for most cases; partner hospital for severe | Separate referral, often a different facility |
| Peer support | Full-time shared milieu | Group sessions only |
| Completion rate (U.S. data) | ~65% (Stahler 2016) | ~52% (Stahler 2016) |
| Best fit | Moderate-severe addiction, failed outpatient, unstable home, co-occurring conditions | Mild addiction, strong sober support, stable housing, must keep working |
What I see clinically is that residential isn’t magic — it’s compression. We deliver the dose research says you need in weeks rather than asking you to do it part-time over a year. For someone with moderate-to-severe dependence, that compression is often the difference between completing treatment and dropping out.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Not sure if inpatient is the right level of care for you? Talk to our team — we’ll give you a straight answer, including if outpatient would serve you better.
What Are the Honest Trade-offs of Inpatient Rehab?
Inpatient costs more upfront, takes you out of work and family life for weeks, and isn’t the right fit for everyone. The trade-off is that you get the treatment dose research says actually works, in the time it takes to deliver it. Most clients who try outpatient first and fail eventually come to inpatient anyway, which makes the cost calculation different than it first looks.
The real trade-offs are concrete:
- Time away from work. 28 to 90 days off. For some clients this is a barrier; for others, employer support or medical leave covers it.
- Family separation. Spouses and children are at home while you’re in treatment. We run family video sessions and an optional family week to bridge this — see our family programme.
- Cost. Higher upfront than outpatient. But factor in failed attempts — outpatient relapse usually means returning to residential later, paying twice.
- Disruption to routine. This is also the point. The routine you have is part of what’s keeping the addiction alive.
We tell clients these limitations openly because if any of them is a deal-breaker for your situation, outpatient (with strong sober supports) may be the right call. Our companion guide compares both formats in detail — inpatient vs outpatient rehab walks through the decision.

What Does Inpatient Rehab at One Step Actually Look Like?
One Step is a 28-to-90-day residential programme in Chiang Mai, Thailand, with a structured day starting at 7am and a clinical team that handles detox, therapy and aftercare planning as one continuous process. We charge approximately ฿280,000 per month (around $8,500 USD), which covers accommodation, three meals, daily therapy, group sessions, exercise, excursions, and assessment with our visiting psychiatrist.
What’s actually on the day:
- 7:00am — Wake, light exercise or meditation
- 8:00am — Breakfast together
- 9:00am–12:00pm — Group therapy and one-to-one counselling
- 12:00pm — Lunch
- 1:30–4:00pm — Skills group (CBT, DBT, relapse prevention)
- 4:00pm — Sports, swimming, or outdoor activity
- 6:30pm — Dinner
- 8:00pm — Evening meeting (12-step format optional)
- 10:30pm — Lights out
See the full treatment schedule, the programme overview, and our activities and excursions for what off-clinic hours look like.
What the fee covers and what it doesn’t. The ฿280,000 monthly fee includes accommodation, food, daily clinical care, intake assessment, and routine progress checks with the visiting psychiatrist. It does not include: medication prescribed during your stay (you pay for what the doctor prescribes), flights, visas or visa extensions, nutraceutical supplements, hospital visits, additional counselling sessions beyond the programme, additional massage or spa sessions, transportation for non-treatment activities, and personal items. For severe withdrawal cases requiring medical detox at our partner hospital before transfer, those hospital fees are also separate. Full breakdown on our pricing page.
How we measure outcomes. Completion rate, dropout reasons, and 6-month and 12-month follow-up contact are the metrics that matter most to us. We don’t promise a number on the website because outcome statistics in the rehab industry are notoriously gameable — but we do tell prospective clients on enquiry calls what we see in practice.
After residential. Continuing care is the single strongest predictor of staying clean beyond a year. Our aftercare programme sets up weekly check-ins, links to local meetings, and a relapse prevention plan before you leave. See also our piece on the 10 most common relapse triggers and how to plan for each — every client builds one of these plans before discharge.
Frequently Asked Questions
Common questions about inpatient substance abuse rehab.
Most inpatient programmes run 28 to 90 days. NIDA’s research-based guidance states that fewer than 90 days of treatment is of limited effectiveness for most substance use disorders. At One Step we recommend a minimum 28-day stay, with most clients choosing 60 or 90 days based on severity and history.
For moderate-to-severe addiction, yes — measured by treatment completion and post-treatment substance use. A 2016 U.S. analysis found residential completion rates near 65% versus 52% for outpatient, and after adjusting for severity, residential clients were nearly three times more likely to complete. Outpatient remains a good fit for mild addiction with strong home support.
Standard inpatient rehab includes accommodation, meals, medical detox where needed, individual and group therapy, psychiatric assessment, and aftercare planning. At One Step the ฿280,000 monthly fee covers all of that plus exercise sessions and excursions. Medication prescribed by the doctor, flights, and visas are billed separately.
Yes. Most inpatient rehabs handle detox on-site for stimulants, cannabis, ketamine, mild-to-moderate alcohol use, and similar substances. For severe alcohol, benzodiazepine, or opioid dependence requiring ICU-level monitoring, One Step refers clients first to our partner hospital — which has intensive and intermediary intensive care units — then transfers them to us for the rehab programme.
Inpatient is not the right fit for very mild addiction with strong sober supports at home, for active psychiatric crisis requiring a locked hospital ward, or for someone who genuinely cannot take time away from caregiving responsibilities. In those cases, intensive outpatient or specialist hospital settings are usually a better starting point.
Some international and private health insurance policies cover overseas residential treatment, especially when domestic options have been tried or are unavailable. Coverage varies widely. We provide the documentation clients need to claim, but reimbursement is between you and your insurer — we recommend confirming coverage in writing before booking.
Continuing care is the strongest predictor of staying clean past the first year. McKay’s review of 20 trials found that longer, more active continuing care produced the best outcomes. At One Step every client leaves with a written relapse prevention plan, a continuing-care schedule, and weekly check-ins through our aftercare programme.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn