Key Takeaways
- CBT for dual diagnosis means one shared formulation linking the mental health condition and the substance use, not two parallel treatments that ignore each other.
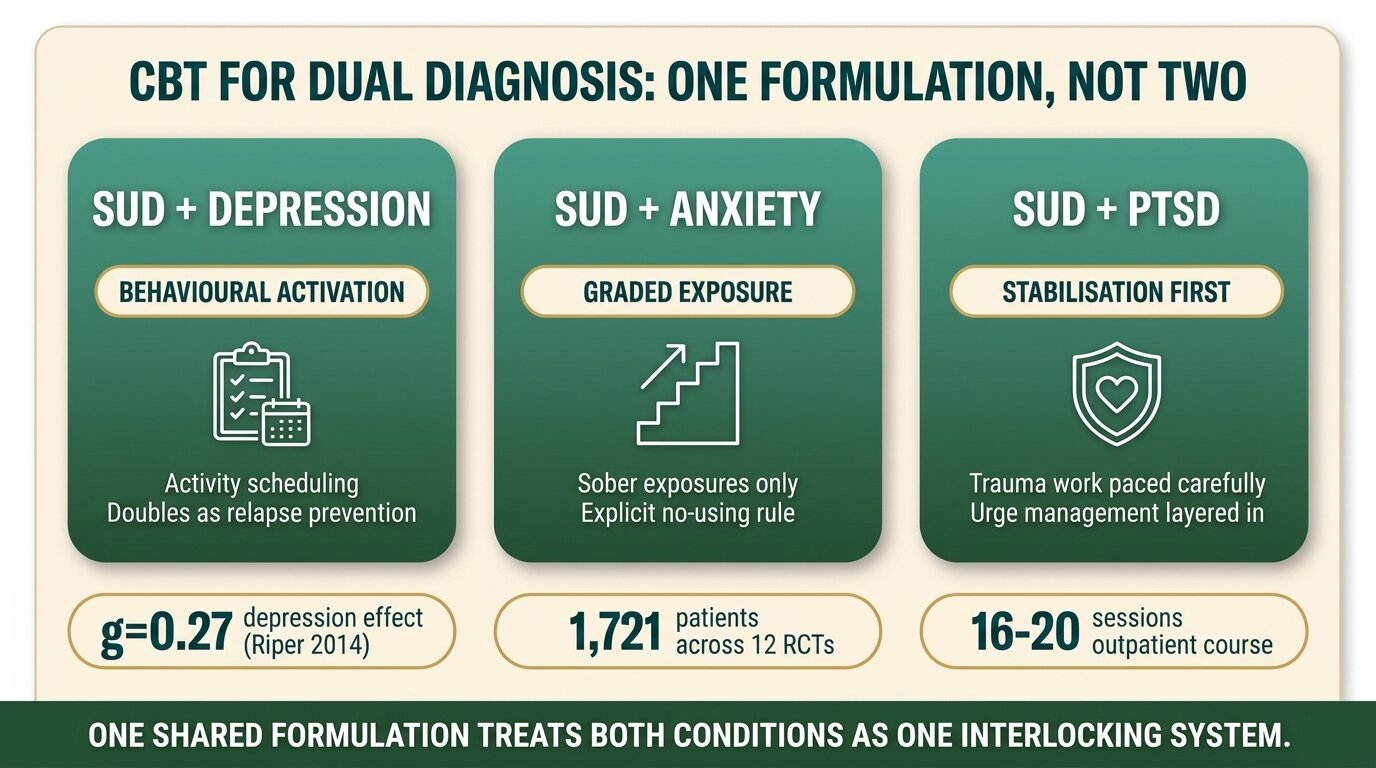
- The session structure shifts depending on the pairing: SUD+depression leads with behavioural activation, SUD+anxiety leads with exposure, SUD+PTSD layers trauma-focused work onto urge management.
- Homework is non-negotiable. CBT works because clients practise skills between sessions — thought records, activity logs, urge surfing diaries. Without homework, CBT becomes talk therapy.
- The Riper 2014 meta-analysis of 12 trials (n=1,721) found CBT and motivational interviewing reduced both alcohol use and depression symptoms in comorbid clients (Riper et al., Addiction, 2014).
- CBT is not optimal for everyone. Trauma-driven cases often need EMDR or trauma-focused CBT layered in; severe borderline personality disorder needs DBT as the spine, with CBT supporting.
CBT for dual diagnosis adapts standard cognitive behavioural therapy so the substance use and the mental health condition are treated as one interlocking problem, not two. A single case formulation maps how depression, anxiety, or PTSD feeds the substance use, and how the substance use sabotages mental health recovery. Session structure, homework, and skill targets all change based on the pairing. Standard CBT alone — built for one disorder at a time — misses the substance use feedback loop and routinely fails dual diagnosis clients (SAMHSA TIP 42, 2020).
Why Does Standard CBT Alone Fail in Dual Diagnosis?
Standard CBT was built for one disorder at a time. When a client has depression and an alcohol use disorder, treating the depression in isolation misses that alcohol is sedating the depression every night — and that the hangover is deepening the depression every morning. Without addressing the substance use feedback loop, the depression protocol stalls, and the client appears “treatment-resistant” when the problem is structural.
This is the trap most general mental health services fall into. A client presents with anxiety, gets referred for CBT, completes 12 sessions of standard anxiety-focused work, and relapses or never improves — because nobody mapped how the daily benzodiazepine use was both maintaining the anxiety (rebound anxiety between doses) and blunting the exposure work. The Carroll and Onken review of behavioural therapies makes the same point: dual diagnosis requires integrated targets, not parallel ones (Carroll and Onken, American Journal of Psychiatry, 2005).
NICE guidance on coexisting severe mental illness and substance misuse takes the same position: services should adapt existing care to meet both sets of needs together rather than running two disconnected pathways (NICE NG58, 2016).
What Is an Integrated Case Conceptualisation?
An integrated case conceptualisation is a single CBT formulation that maps the mental health condition and the substance use as one interlocking system. It identifies how each maintains the other, where the loops break open, and what intervention sequence will actually disrupt the cycle. One formulation, one treatment plan — not two separate workbooks sitting side by side.
In practice, this looks like a flowchart drawn with the client in the second or third session. For someone with depression and alcohol dependence, it might map: low mood and rumination at 6pm → reach for alcohol to numb out → drink past intended limit → wake with hangover and guilt → reduced activity the next day → deeper low mood → 6pm trigger returns. The formulation makes the loop visible. From there, the therapist and client decide which loop point is most workable: the 6pm trigger, the urge to numb, the morning recovery, or the missed activities.
The formulation also names the unhelpful beliefs that bridge the two conditions — beliefs like “alcohol is the only thing that quiets my head” (a permission-giving belief about substance use that is reinforced by the actual depressive symptoms), or “if I stop drinking, the anxiety will be unbearable” (a catastrophic belief that ties relapse risk directly to the mental health condition). Standard CBT for depression would address depressive thoughts. Standard CBT for SUD would address substance-related thoughts. Integrated CBT addresses the beliefs that span both.
How Does CBT Structure Change by Dual Diagnosis Pairing?
The CBT structure shifts depending on which mental health condition is paired with the substance use. SUD+depression leads with behavioural activation and pairs it with relapse prevention. SUD+anxiety leads with exposure work but adapts it so it doesn’t trigger substance use. SUD+PTSD layers trauma-focused techniques onto urge management. The skeleton is recognisably CBT — the sequencing and the skill emphasis are different.
SUD plus depression
Behavioural activation is the spine. The client commits to scheduled, valued activities that gradually rebuild the reinforcement that depression has stripped out. The substance-related layer is that many of these activities have to be planned around high-risk drinking or using times — so the activity schedule and the relapse-prevention plan are drawn up together. A 6pm gym session is both a behavioural activation move and a relapse prevention move. The Riper meta-analysis specifically supports CBT combined with motivational interviewing for this pairing, with small but consistent effects on both alcohol consumption and depression symptoms across 12 trials and 1,721 patients (Riper et al., Addiction, 2014).
SUD plus anxiety
Exposure work is central — but the therapist has to plan exposures so the client doesn’t substance-use through them. A client with social anxiety who normally drinks before social exposure has to do graded exposures sober. That means smaller exposure steps at the start, longer practice at each step, and an explicit “no using before, during, or after” rule for each exposure assignment. Standard CBT for anxiety would just prescribe the exposure ladder. Integrated CBT prescribes the ladder plus the using rules plus an in-session plan for what to do when the urge to use spikes during exposure homework.
SUD plus PTSD
This is the hardest pairing to structure. Trauma-focused work risks destabilising clients who use substances to manage trauma symptoms. Integrated CBT here either sequences (stabilisation and substance use work first, then trauma processing) or runs concurrently with careful pacing. Some clients do better with trauma-focused CBT or EMDR layered into the dual diagnosis treatment; others need the SUD locked down for several months before any trauma processing begins. The NIDA-supported integrated CBT trials for PTSD plus SUD show this pairing benefits from treating both as one syndrome rather than sequencing them years apart (McGovern et al., Addiction, 2011).
SUD plus other conditions
Bipolar disorder, OCD, and eating disorders each have their own integrated CBT considerations. The principle is the same: one formulation, one treatment plan, skill targets that address both conditions at once. The session skeleton stays CBT — agenda setting, skill teaching, homework review, homework setting — but the skill content varies.
| Pairing | Lead technique | Key adaptation | Common failure point |
|---|---|---|---|
| SUD + depression | Behavioural activation | Activity scheduling doubles as relapse prevention | Treating depression in isolation; client keeps drinking through BA homework |
| SUD + anxiety | Graded exposure | Exposures done sober; explicit “no using” rule per assignment | Client uses to get through exposure homework, learns nothing |
| SUD + PTSD | Trauma-focused work plus urge management | Stabilisation often comes first; trauma processing paced carefully | Either avoiding trauma forever or pushing into it before SUD is stable |
| SUD + bipolar | Mood monitoring plus relapse prevention | Identifying substance use as both trigger and consequence of mood episodes | Treating manic-phase substance use as the “real” problem and missing the mood episode |

Why Is Homework Discipline So Important in CBT for Dual Diagnosis?
CBT works because clients practise skills between sessions. Thought records, activity logs, urge surfing diaries, and behavioural experiments are where the actual change happens — the session is where you learn the skill and review last week’s practice. In dual diagnosis, the homework load is heavier because there are usually two skill tracks running at once: one for the mental health condition and one for the substance use. Skip the homework and CBT becomes weekly talk therapy with a structured agenda.
The non-negotiable homework types in integrated CBT are: a daily mood and urge log (tracks both conditions in one place), a thought record for the unhelpful beliefs the formulation identified, and at least one behavioural experiment or activity assignment per week. In residential treatment this is easier to enforce because the structure of the day creates protected time for homework completion. In outpatient settings, homework completion is the single biggest predictor of who improves and who doesn’t.
The clients who do well in integrated CBT are the ones who show up to session two with the homework done. Not perfectly — just done. We can work with imperfect homework. We can’t work with no homework. When someone tells me they “didn’t have time” three weeks running, that’s not a homework problem, that’s a formulation problem — we haven’t yet found the loop point that matters to them.
David KaffSenior Therapist, One Step Rehab
Wondering whether integrated CBT is the right approach for your situation? Talk to our team — we’ll give you a straight answer, including if we think a different therapy fits you better.
What Does the Evidence Actually Say About CBT for Dual Diagnosis?
The evidence base for CBT in dual diagnosis is solid but not spectacular. Effect sizes are small to moderate, comparable to other evidence-based modalities, with the strongest support for SUD plus depression and SUD plus anxiety. CBT is not the only therapy that works — but it is one of the best-studied, and the integrated versions outperform parallel treatment in the trials that exist.
The Riper 2014 meta-analysis pooled 12 randomised controlled trials of CBT plus motivational interviewing for alcohol use disorder with major depression. Across 1,721 patients, the combined approach produced small but reliable effects — Hedges’ g = 0.17 for reduced alcohol consumption and g = 0.27 for reduced depressive symptoms at post-treatment. Digital interventions actually outperformed face-to-face for depression in this sample (Riper et al., Addiction, 2014).
Magill and Ray’s broader meta-analysis of 53 CBT trials for alcohol and drug use disorders found a similar small overall effect (g = 0.15) when CBT was compared with other active treatments, and a large effect (g = 0.79) when compared with no treatment. The implication is important: CBT clearly beats nothing, but it doesn’t clearly beat other well-delivered evidence-based therapies for SUD in general samples (Magill and Ray, Journal of Studies on Alcohol and Drugs, 2009).
Hofmann’s review of meta-analyses across 106 reviews found CBT broadly effective across mental health conditions, with the strongest evidence for anxiety disorders, depression, and bulimia, and good evidence for substance use disorders specifically (Hofmann et al., Cognitive Therapy and Research, 2012). For PTSD plus SUD specifically, McGovern’s trial showed integrated CBT outperformed standard addiction counselling for reducing PTSD re-experiencing symptoms (McGovern et al., Addiction, 2011).

When Is CBT Not the Right Choice for Dual Diagnosis?
CBT is not the right first-line treatment for everyone with dual diagnosis. Trauma-driven cases often respond better to EMDR or trauma-focused CBT than to standard CBT. Severe borderline personality disorder usually needs DBT as the structural spine, with CBT techniques supporting. Active psychosis, untreated severe ADHD, and certain cognitive impairments make the homework discipline of CBT extremely difficult to sustain.
The honest decision rule we use: if the client’s primary mental health condition is trauma and the substance use is mostly a coping response to trauma symptoms, we lean on EMDR or trauma-focused CBT rather than general integrated CBT. We have a separate guide to the differences between CBT and DBT for addiction that goes deeper into when DBT is the better spine.
For clients with severe BPD plus SUD, DBT is usually the structural treatment of choice because its skill modules (distress tolerance, emotion regulation, interpersonal effectiveness, mindfulness) map directly onto the deficits that drive both the BPD symptoms and the substance use. CBT techniques can be brought in around the edges, but they’re not the spine. For active psychosis, the priority is psychiatric stabilisation first — CBT for psychosis (CBTp) is well-evidenced, but it’s a specialist adaptation rather than the integrated CBT we’re describing here.
How Does CBT for Dual Diagnosis Work at One Step?
At One Step, CBT for dual diagnosis is delivered inside our residential programme by senior therapists trained in the Beck-style CBT model and adapted for substance use work. Clients have several individual sessions per week and CBT-informed group work daily. The integrated case formulation is built in the first week and revisited throughout treatment. Homework is structured into the daily schedule.
The residential structure is the reason the homework discipline holds. In an outpatient setting, a client with depression and alcohol use disorder might finish a session, intend to do their activity scheduling and thought records, then drink that night and miss everything. In our residential programme, there’s no alcohol available, the activity schedule is the day itself (gym, group, outdoor therapy, structured downtime), and homework review happens in the next morning’s session before momentum is lost.
The programme runs at ฿280,000 per month (approximately $8,500 USD) for a typical 28-day stay, with most clients staying 30 to 60 days. That fee covers accommodation, food, all therapy sessions, group work, and on-site clinical support. Pricing details are on a separate page. Medication is billed separately — if our visiting psychiatrist prescribes an antidepressant, mood stabiliser, or anxiolytic as part of your dual diagnosis treatment, you pay for the medication itself, the same way you’d pay for flights or visa fees.
For clients arriving with severe alcohol, benzodiazepine, or opioid dependence requiring medical detox beyond what a residential rehab can provide, we may arrange detox first at our partner hospital — which has intensive and intermediary intensive care units — before you transfer to One Step for the CBT-based dual diagnosis programme. For most dual diagnosis cases without severe withdrawal complications, detox is handled on-site at One Step.
We are not a locked psychiatric facility. For dual diagnosis clients in active psychosis, acute suicidal crisis, or requiring involuntary admission, hospital-based care is the appropriate first step. We accept clients once they are medically and psychiatrically stable enough for residential treatment. Our dual diagnosis programme, personalised therapy options, and types of dual diagnosis therapies guides cover the wider treatment context.
How Do Behavioural Activation and Relapse Prevention Work Together?
Behavioural activation and relapse prevention are the two CBT techniques that most often run side by side in dual diagnosis. Behavioural activation gets the depressed client doing valued, scheduled activities again. Relapse prevention identifies high-risk situations and builds skills to navigate them without using. When they’re integrated, the activity schedule itself becomes the relapse prevention plan.
An example from a typical SUD+depression case: a client’s high-risk drinking time is 6pm to 10pm at home alone, and their behavioural activation targets are “more time outdoors” and “rebuild gym habit.” The integrated plan books gym sessions at 6:30pm three nights a week — solving both problems in one move. The activity earns the behavioural activation points (rebuilding reinforcement) and removes the client from the high-risk drinking environment at the exact danger window. Standard CBT for depression might just say “schedule pleasant activities.” Integrated CBT picks the activities that double as relapse prevention.
The homework around this is a daily log with three columns: mood rating, urge rating, and what activity was done. Over two to three weeks, patterns emerge — which activities reliably lift mood and reduce urges, which don’t, what time of day is hardest, where the activity schedule needs to be tightened. The therapist and client use the log to refine the plan week by week.
Frequently Asked Questions
Common questions about CBT for dual diagnosis treatment.
Yes, with caveats. Meta-analytic evidence supports CBT for SUD plus depression and SUD plus anxiety with small-to-moderate effect sizes. Integrated CBT (one formulation, one plan) outperforms running two separate treatments in parallel. CBT works less well as a sole treatment for trauma-driven dual diagnosis or severe BPD-plus-SUD, where EMDR or DBT may be better suited.
Standard CBT treats one disorder. Integrated CBT for dual diagnosis uses one shared case formulation that maps how the mental health condition and the substance use maintain each other, with skill targets that address both at once. Activity schedules double as relapse prevention. Thought records target beliefs that span both conditions.
Outpatient courses typically run 16 to 20 weekly sessions for SUD plus depression or anxiety. Residential programmes compress this — at One Step, clients receive several individual CBT sessions per week plus daily CBT-informed group work over 30 to 60 days. Trauma-focused dual diagnosis work often takes longer because the trauma processing component needs careful pacing.
CBT itself is talking therapy and does not include medication, but most dual diagnosis treatment plans combine CBT with psychiatric medication where indicated — antidepressants for SUD plus depression, SSRIs for SUD plus anxiety, mood stabilisers for SUD plus bipolar disorder. Medication and CBT work together. At One Step, medication costs are billed separately from the programme fee.
It depends on the pairing. CBT tends to be the better spine for SUD with depression, anxiety, or PTSD. DBT tends to be the better spine when borderline personality disorder, severe emotion dysregulation, or chronic self-harm are part of the picture. Many programmes use CBT as primary and pull in DBT skill modules where needed.
CBT works because clients practise skills between sessions. Thought records, activity logs, and urge surfing diaries are where the actual cognitive and behavioural change happens. In dual diagnosis the homework load is heavier because there are usually two skill tracks running. Without consistent homework completion, CBT becomes weekly talk therapy with a structured agenda.
Yes. The Riper 2014 meta-analysis found that digital CBT and motivational interviewing interventions for alcohol use disorder with depression actually produced larger effect sizes for depression symptoms than face-to-face delivery in the same trials. Online CBT works best for mild-to-moderate dual diagnosis. Severe cases, active suicidality, or unstable substance use generally still need in-person residential or intensive outpatient care.
Written by
David Kaff
David Kaff is an Addictions Counselor with over a decade of experience working in both harm reduction and residential treatment settings in Australia and Thailand. He has worked across frontline services, 12-step based r...
Learn more about David
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn