Key Takeaways
- EMDR (Eye Movement Desensitisation and Reprocessing) is one of two trauma therapies the WHO and NICE recommend for PTSD — the other is trauma-focused CBT.
- For people whose addiction is medicating untreated trauma, EMDR can break a ceiling that talk therapy keeps hitting. It is not a cure for addiction.
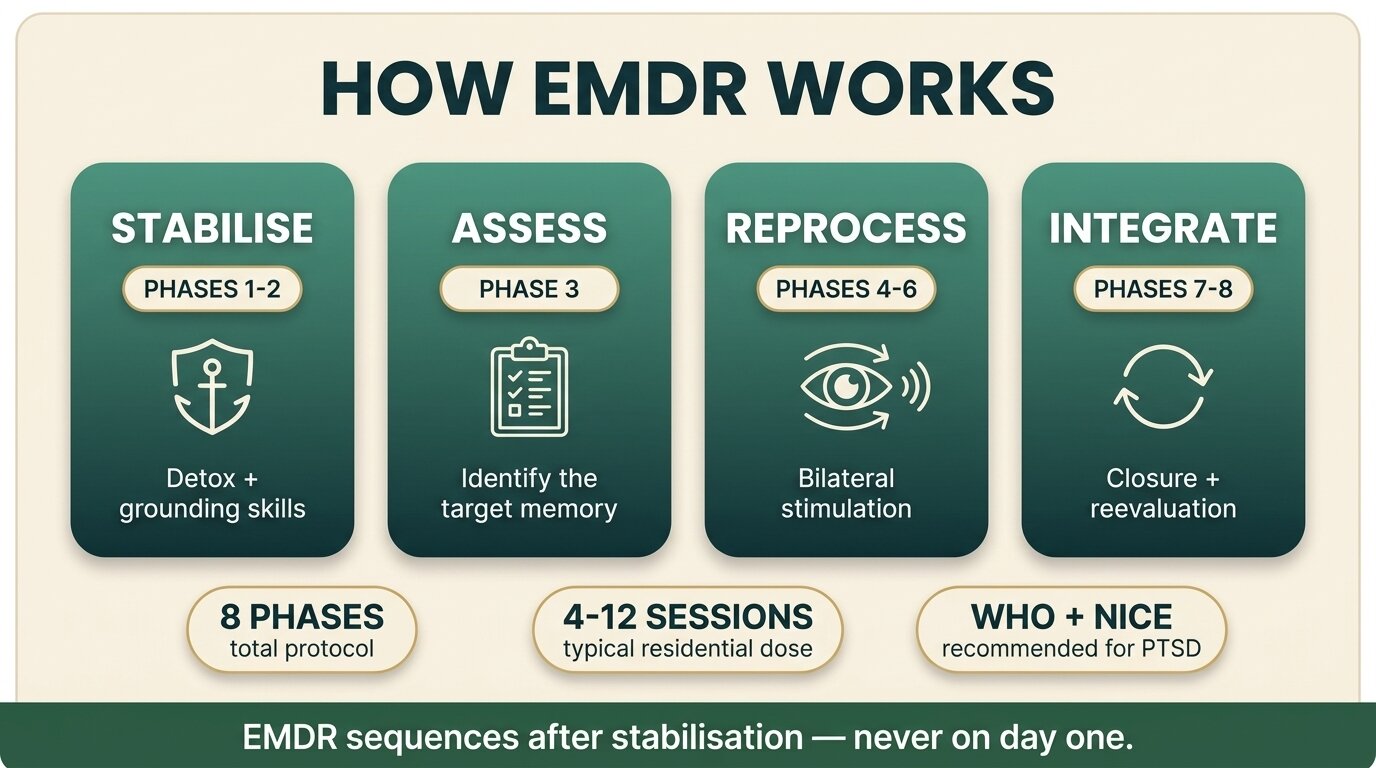
- EMDR uses bilateral stimulation (eye movements, taps, or tones) while the client briefly recalls a traumatic memory. The protocol has 8 phases — most of the visible work happens in phases 3 to 6.
- Stabilisation comes first. EMDR is sequenced after detox and after initial coping skills are in place, not on day one of treatment.
- At One Step, EMDR is used for clients with PTSD plus substance use disorder after the initial stabilisation phase — typically 4 to 12 sessions during the residential stay, with continued work in aftercare for some.
EMDR is a trauma-focused psychotherapy that helps the brain reprocess stuck traumatic memories so they stop driving present-day symptoms — including the cravings and avoidance that fuel addiction. The World Health Organization recommends it as one of only two evidence-based therapies for adult PTSD, alongside trauma-focused CBT (WHO, 2013). NICE in the UK gives it the same standing for adults presenting more than three months after a non-combat trauma (NICE NG116, 2018). It is not magic, it is not for everyone, and the order of treatment matters. Here is what EMDR actually involves, what the evidence says for people with PTSD plus a substance use disorder, and where it fits at One Step.
What Is EMDR and How Does It Work?
EMDR is a structured eight-phase psychotherapy in which the client briefly holds a distressing memory in mind while a therapist guides them through bilateral stimulation — usually side-to-side eye movements, but also taps or alternating tones. The working theory is that the bilateral stimulation mimics the memory-processing that happens in REM sleep, letting the brain re-file the memory as a past event rather than a present threat.
Francine Shapiro developed the protocol in the late 1980s. Since then, around forty controlled trials have tested it for PTSD. A Cochrane review of psychological therapies for chronic PTSD found that EMDR and trauma-focused CBT both outperformed waitlist and usual-care controls on clinician-assessed PTSD symptoms, with comparable effect sizes (Bisson et al., Cochrane Database, 2013). That is why the WHO and NICE list them as the two front-line trauma therapies.
There is a real scientific debate about why EMDR works. Some researchers argue the bilateral stimulation itself is the active ingredient. Others argue it is essentially imaginal exposure with a dual-attention task layered on top. The outcome data for PTSD is robust either way. The mechanism debate is ongoing and does not undermine the clinical evidence.

Why Does EMDR Matter Specifically for Addiction?
EMDR matters in addiction treatment because a significant share of people with substance use disorder are medicating untreated trauma. When the trauma stays untreated, traditional addiction therapy often hits a ceiling: the client gets the coping skills, but the memory keeps firing, and the relief from substances stays seductive. EMDR can reprocess the memory so the urge to medicate it loses force.
The overlap between PTSD and substance use disorder is large. Roughly 20 to 35 percent of people with PTSD also have a substance use disorder, and 30 to 60 percent of people in treatment for substance use disorders meet criteria for PTSD (Hien et al., Frontiers in Behavioral Neuroscience, 2020). Combat veterans, sexual assault survivors, adults with childhood trauma, and first responders carry that overlap into rehab admissions in numbers most outsiders underestimate. For this group, treating the addiction without addressing the trauma is treating half the problem.
The evidence base for EMDR specifically in dual diagnosis is younger and thinner than the PTSD evidence base, but it is growing. Carletto and colleagues ran an add-on trial — 24 weekly EMDR sessions on top of treatment-as-usual versus treatment-as-usual alone — and found significantly greater reductions in post-traumatic and dissociative symptoms in the EMDR group, though abstinence rates were similar (Carletto et al., Frontiers in Psychology, 2018). A 2024 meta-analysis of five trials covering 266 participants found EMDR significantly reduced craving in people with substance use disorders, with a large pooled effect size (Martínez-Fernández et al., Brain Sciences, 2024). Most recently, a large four-arm randomised trial in the Netherlands compared EMDR, prolonged exposure, and imagery rescripting added to standard SUD treatment, with 209 patients across two addiction centres (Lortye et al., Addiction, 2025).
The honest summary: EMDR helps PTSD symptoms in people who also have a substance use disorder, and there is reasonable evidence it helps with craving too. It does not directly “treat addiction” the way naltrexone treats opioid dependence or CBT for substance use teaches relapse-prevention skills. What it does is dissolve the trauma layer that often sits underneath the substance use, which can change everything else.
What Are the Eight Phases of EMDR?
EMDR follows an eight-phase protocol that runs from history-taking through reprocessing to reevaluation. The visible “eye movement” piece happens in phases 3 to 6. Phases 1 and 2 are preparation — the part many clients skip in their imagination but which is non-negotiable in practice, especially in dual diagnosis. Phase 7 closes the session safely and phase 8 checks the work has held.
| Phase | Name | What happens |
|---|---|---|
| 1 | History & treatment planning | Therapist takes a trauma history, screens for dissociation and stability, and identifies target memories. |
| 2 | Preparation | Builds rapport, explains the model, teaches grounding and self-soothing skills (e.g. the “safe place” exercise). |
| 3 | Assessment | Client identifies the worst image, the negative belief tied to it, a target positive belief, and current body sensations. |
| 4 | Desensitisation | Bilateral stimulation begins. The client briefly notices the memory, then follows the therapist’s fingers (or taps, or tones). The therapist pauses, asks “what comes up?”, and repeats. |
| 5 | Installation | The positive belief is paired with the now-less-charged memory and reinforced with further bilateral sets. |
| 6 | Body scan | Client scans the body for residual tension or sensation linked to the memory; remaining charge is reprocessed. |
| 7 | Closure | Session is closed safely whether or not reprocessing is complete; grounding skills are re-engaged before the client leaves the room. |
| 8 | Reevaluation | Next session, therapist checks whether gains held, looks for new material, and adjusts targets. |
Most clients spend more time in phases 1 and 2 than they expect. In a dual-diagnosis setting that preparation often takes weeks, not a single appointment. Skipping it is how EMDR goes badly.

What Does an EMDR Session Actually Feel Like?
An EMDR session feels less like talking therapy and more like watching a film of your own memory at someone else’s pace. You hold the target memory in mind, follow the therapist’s hand or the tones, and then they pause and ask “what comes up?” Whatever surfaces — a new image, a body sensation, an old memory you had forgotten — becomes the next target. The work is internal. You are not telling a long narrative.
People often report that the memory shifts in emotional charge across a session. Something that started at an 8 out of 10 in distress drops to a 2 or 1. The image itself does not disappear. What changes is its grip. Clients describe it as the memory “moving from front to back” or finally feeling “like it happened, instead of like it is happening.” Some sessions feel uneventful and reprocessing only lands later. Some sessions feel like a wave breaking. Both are normal.
The clients who get the most out of EMDR are usually the ones who came in convinced talk therapy was not reaching the thing underneath. The trauma had a grip the words could not touch. What we see, when the stabilisation work has been done first, is that the memory loses its power to dictate the day. The craving for whatever they were medicating with quiets in a way they have not felt before.
Craig GagnonSenior Therapist, One Step Rehab
Who Is EMDR For — and Who Should Wait?
EMDR is a strong fit for adults with a discrete traumatic memory or a clear PTSD picture — intrusive memories, avoidance, hyperarousal — particularly when talk therapy has stalled or never reached the trauma. It works well in dual diagnosis once the substance use has stabilised. It is not for everyone, and the contraindications are taken seriously by any competent practitioner.
| Good candidate if | Caution or wait if |
|---|---|
| Clear PTSD diagnosis with intrusive memories and avoidance. | Active psychosis or untreated psychotic illness. |
| Discrete trauma memory or identifiable cluster (assault, accident, combat, specific abuse event). | Severe dissociation that has not been screened and addressed. |
| Substance use is in early remission and stabilisation skills are in place. | Active heavy substance use — reprocessing without sobriety is destabilising. |
| Talk therapy has helped, but the trauma layer is still firing. | Complex C-PTSD without prior phase-based stabilisation work. |
| Client can tolerate distress for short blocks (90 seconds at a time). | Severe self-harm or active suicidal crisis — stabilise first. |
“Wait” does not mean “never.” Most contraindications mean “do the stabilisation work first, then come back to EMDR.” That sequencing is the difference between EMDR helping and EMDR backfiring.
Why Does Stabilisation Have to Come First?
Stabilisation has to come first because reprocessing a traumatic memory means temporarily turning the volume up before it goes down. If the client is in active withdrawal, severely dissociating, or without coping skills, the temporary spike can drive relapse, dissociative collapse, or a crisis. Phase 2 of the EMDR protocol — preparation — exists specifically to build the floor before the trauma work begins.
In practice that means: detox first, then a few weeks of group work, individual sessions, sleep stabilisation, basic grounding skills (the “safe place” exercise, bilateral resourcing, breath work), and an assessment of dissociation risk. Only then does EMDR’s desensitisation phase begin. A therapist who runs phase 4 on day three of a residential stay is not following the protocol — they are improvising, and the client is the one who pays for it.
This sequencing is also why EMDR sits inside a wider treatment plan rather than functioning as a stand-alone intervention. It complements — and is complemented by — CBT and DBT, individual addiction counselling, and group work. In dual diagnosis cases, it is one tool in a sequenced plan, not the whole plan.
Not sure if EMDR is the right fit for your situation? Talk to our team — we will tell you honestly, including if we think a different approach would serve you better.

How Does One Step Use EMDR in Treatment?
At One Step, EMDR is delivered by therapists trained in the protocol and used for clients with PTSD plus a substance use disorder after the initial stabilisation phase of the residential programme. Not every client gets EMDR — it is matched to a specific case formulation based on the intake assessment. For those who are good candidates, the typical pattern is 4 to 12 reprocessing sessions during the residential stay, with continued sessions in aftercare for clients with complex trauma histories.
The sequencing inside our programme runs roughly like this. Clients arrive, go through detox (on-site for most substances), and spend the first phase of treatment in group work, individual counselling, and skills-building — including the grounding and coping work that doubles as EMDR phase 2 preparation. Trauma assessment happens during this period. If EMDR is indicated, reprocessing sessions begin once the floor is stable, typically several weeks in. The rest of the residential schedule continues alongside — group therapy, fitness, outdoor therapy, activities — so EMDR is one strand of the day, not the whole day.
For clients whose addiction is fundamentally trauma-driven, EMDR often becomes the piece that the rest of the work was missing. For clients whose addiction does not have a clear PTSD component, EMDR is not pushed. Our broader approach to personalised dual diagnosis therapy options and the wider range of dual diagnosis therapies we use is built around matching the right intervention to the right person, not running every client through the same protocol.
The residential fee covers the therapy, the room, the food, and the structured programme (see pricing for the full list). Medication, flights, visas, hospital visits, and personal items are billed separately. EMDR sessions during the residential stay are part of the programme; continued EMDR in aftercare is arranged separately if needed. Our treatment programme and treatment schedule pages describe how the daily structure fits together. Our broader dual diagnosis treatment page covers the wider approach for clients with co-occurring conditions, and aftercare covers what comes after discharge.
If you or someone you love is struggling with substance dependence, explore how a drug addiction treatment programme can provide the structure, clinical support, and environment needed for lasting recovery.
EMDR and Addiction: Frequently Asked Questions
Short answers to the questions readers most often ask before deciding whether EMDR is right for them.
The outcome evidence for EMDR in PTSD is strong. Both the WHO and NICE list it as one of two front-line trauma therapies alongside trauma-focused CBT. What is still debated in the research is the mechanism — whether the bilateral stimulation itself is the active ingredient or whether EMDR works through exposure with a dual-attention task. The clinical results hold either way.
No therapy “cures” addiction. EMDR can dissolve the trauma that drives the substance use, which often changes the texture of cravings and avoidance. For people whose addiction is medicating untreated trauma, that shift can be transformative. For people whose addiction is not trauma-driven, EMDR is not the right tool.
For a single discrete trauma, 6 to 12 sessions is typical. For complex trauma with multiple memories, more sessions are needed and stabilisation work takes longer up front. At One Step, most clients receive 4 to 12 reprocessing sessions during a residential stay, with continued work in aftercare if the trauma history is layered.
The distress level on a memory typically rises briefly during a reprocessing session before dropping. This is why stabilisation, grounding skills, and a tolerant therapeutic relationship are built in phase 2 before reprocessing begins. Between sessions, some clients have vivid dreams or surfacing memories — these are usually signs the brain is working, not a setback.
EMDR reprocessing is sequenced after detox and after initial coping skills are established. It is not started on day one. A few weeks of stabilisation is the standard before phase 4 begins. This protects against the temporary distress spike during reprocessing destabilising new sobriety.
Yes. EMDR does not require a verbal narrative of the memory. The target can be a fragment, an image, a body sensation, or a feeling. The client does not have to tell the therapist what happened in detail for reprocessing to work. This makes EMDR accessible for clients whose trauma is held more in the body than in coherent recollection.
Yes. We have therapists trained in EMDR and use it for clients with PTSD plus substance use disorder after the initial stabilisation phase of treatment. EMDR is matched to specific case formulations during the intake assessment, not offered to every client. If you want to know whether it is likely to be part of your plan, contact us directly.
Written by
Craig Gagnon
Craig Cagnon is an American counseling psychologist and addiction counselor. He holds Masters degrees in community counseling and counseling psychology and completed his clinical residency at The Mayo Clinic, in Rochest...
Learn more about Craig
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn