
Key Takeaways
- Inpatient alcohol rehab is usually the right call for people drinking heavily for years, anyone with prior withdrawal seizures or delirium tremens, and anyone whose home environment makes outpatient impossible.
- The DSM-5 system grades alcohol use disorder as mild (2–3 criteria), moderate (4–5), or severe (6+). Most severe cases need residential treatment to interrupt the cycle.
- Two of the strongest indicators for inpatient care are a history of failed outpatient detox and three or more prior detoxes — repeated withdrawals get worse, not easier (Becker, Alcohol Health and Research World, 1998).
- Co-occurring depression, anxiety, PTSD, or other mental health conditions roughly double the case for residential treatment over outpatient.
- One Step Rehab in Chiang Mai charges ฿280,000/month (~$8,500 USD) for residential treatment. Severe withdrawal cases detox at our partner hospital first, then transfer to us for the rehab programme.
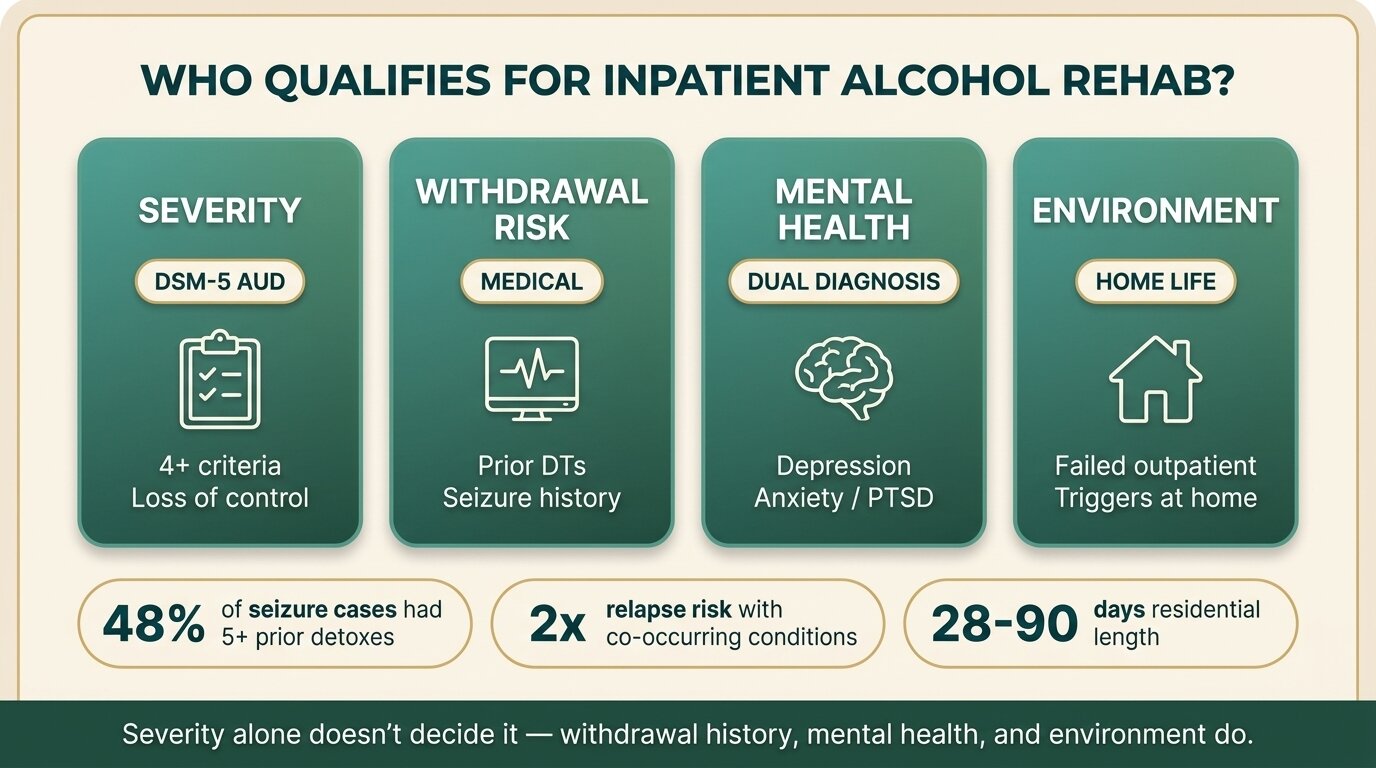
You qualify for inpatient alcohol rehab if your drinking has reached the point where outpatient treatment can’t safely interrupt it. The core indicators are: a daily drinking pattern that has lasted years, a history of withdrawal seizures or delirium tremens (DTs), one or more failed attempts at outpatient detox, a co-occurring mental health condition, or a home environment that keeps you drinking. The DSM-5 framework grades alcohol use disorder as mild, moderate, or severe based on how many of 11 diagnostic criteria you meet — moderate-to-severe AUD almost always warrants residential care (NIAAA, 2024).
This post is a self-assessment guide, not a diagnostic tool. If you recognise yourself in two or three of the indicators below, the question isn’t whether you need inpatient rehab — it’s whether you’re going to make the call now or after the next crisis.
How Severe Does Your Drinking Have to Be?
Inpatient alcohol rehab is generally indicated for moderate-to-severe alcohol use disorder under DSM-5 — meaning four or more diagnostic criteria within a 12-month period. The American Society of Addiction Medicine (ASAM) places severe AUD at Level 3 (residential) or Level 3.7 (medically monitored inpatient) on its placement criteria, while mild AUD usually fits Level 1 outpatient care.
The 11 DSM-5 criteria cover loss of control over drinking, tolerance, withdrawal, neglect of responsibilities, drinking in dangerous situations, and continued use despite known harm. You don’t have to meet all 11 to qualify as severe — meeting 6 puts you there. The honest test isn’t “do I drink too much” but “have I tried to stop and found I can’t”?
| Severity | DSM-5 criteria met | Typical level of care |
|---|---|---|
| Mild AUD | 2–3 | Outpatient counselling, brief intervention |
| Moderate AUD | 4–5 | Intensive outpatient or residential (depends on context) |
| Severe AUD | 6+ | Residential / inpatient rehab |
Severity alone doesn’t decide it. A person with four criteria and a supportive family at home, no withdrawal history, and a stable job may do fine in intensive outpatient. A person with the same four criteria, an alcoholic spouse, two prior detoxes, and an anxiety disorder needs residential. Context is doing most of the work.
What Withdrawal Risk Factors Force the Inpatient Decision?
Several withdrawal risk factors make inpatient rehab the only safe option: a history of seizures or delirium tremens during prior withdrawal, three or more previous detox attempts, drinking more than a litre of spirits or 10+ beers daily for several years, alcoholic liver disease, age over 40 combined with long-term heavy drinking, and concurrent benzodiazepine or opioid use. Any one of these tilts the case toward residential care; two or more makes the decision for you.
The most important risk factor is your withdrawal history. Repeated detoxifications make subsequent withdrawals worse — a phenomenon called “kindling.” In a clinical study, 48% of alcoholics who had seizures during withdrawal had been through 5 or more prior detoxes, compared to 12% of those without seizures (Brown et al., Biol Psychiatry, 1988). Each unsupervised attempt to stop raises the stakes of the next one. If your last home detox involved shaking that wouldn’t stop, hallucinations, or a seizure, the next one will likely be worse — not better.
Delirium tremens carries a mortality risk of roughly 3–5% in untreated cases and develops 48–72 hours after the last drink. The combination of confusion, fever, hallucinations, and autonomic instability is a medical emergency, not something to ride out at home or in a residential facility without hospital-grade monitoring. For severe withdrawal cases, we may detox you first at our partner hospital — which has intensive and intermediary intensive care units — then you transfer to One Step for the rehab programme.
Indicators that point to hospital-based detox before residential rehab
- Prior history of delirium tremens or alcohol withdrawal seizures
- Heavy daily drinking (1+ litre of spirits or equivalent) for several years
- Concurrent benzodiazepine or opioid dependence
- Significant liver damage, advanced age, or a serious co-occurring medical illness
- A failed home or outpatient detox in the last 12 months
One Step handles standard alcohol detox on-site for most clients. The partner hospital referral applies only when withdrawal is severe enough to need ICU-level monitoring — usually the indicators above.

When Does a Co-Occurring Condition Tip the Decision Toward Inpatient?
If you have depression, anxiety, PTSD, bipolar disorder, or another mental health condition alongside heavy drinking, the case for inpatient rehab roughly doubles. Co-occurring conditions make outpatient treatment fragile — the underlying mental health symptoms drive relapse, and unmedicated or unsupported symptoms make engagement in outpatient sessions hard to sustain. Integrated residential treatment addresses both simultaneously.
Among adults with mental illness, around 11 million also have alcohol use disorder, and people with co-occurring conditions are roughly twice as likely to relapse in the months after AUD treatment compared to those with AUD alone (NIDA, 2024). The relapse risk isn’t a verdict on the person — it’s a verdict on fragmented care that treats one condition while leaving the other untouched.
Common patterns we see in admissions:
- Anxiety + alcohol — drinking to take the edge off panic, which generates more anxiety the next day, which generates more drinking. The cycle won’t break with outpatient counselling because the person hasn’t been a day sober in years.
- Depression + alcohol — alcohol is a depressant, but it’s also temporarily an anaesthetic for depressive symptoms. Stopping makes the depression briefly worse before it gets better. Residential makes that crossing survivable.
- PTSD + alcohol — drinking suppresses trauma symptoms. Detox without trauma support reactivates everything at once. CBT and DBT therapy done in residential settings can hold both at once.
If you have a diagnosed mental health condition and your drinking has escalated, the question isn’t whether to do residential — it’s how long. Our dual diagnosis programme integrates psychiatric care with the rehab schedule rather than treating them as separate problems.
The patients I see who do best in residential treatment aren’t necessarily the ones who drink the most. They’re the ones who can’t get a clean week at home no matter how hard they try — usually because of a co-occurring anxiety or depressive disorder, sometimes because of an unstable home life. Severity of drinking tells me what kind of medical detox someone needs. The reason they keep relapsing tells me what kind of treatment they need afterward.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab

How Much Does Your Home Environment Matter?
Home environment is one of the biggest predictors of whether outpatient treatment will work. If you live with someone who drinks, work in a job where alcohol is part of the social fabric, or have easy access to alcohol when cravings hit, outpatient is fighting uphill. Residential treatment removes the environment from the equation for 28–90 days, which is often what makes the difference between a real recovery attempt and another cycle.
The honest checklist:
- Does anyone you live with drink in front of you?
- Is alcohol in the house right now?
- Is your job tied to drinking — hospitality, sales entertainment, certain trades?
- Are your closest friends people you mainly drink with?
- Have you tried to stop at home in the last year and failed within 30 days?
If you answered yes to three or more, your environment is a significant relapse risk. That doesn’t mean outpatient is impossible — it means outpatient is harder, and the structure of residential treatment is doing important work that you’d otherwise have to construct yourself with willpower alone. Most people don’t have that much willpower. That’s not a character flaw; that’s biology.
Not sure where you fit? Talk to our team — we’ll give you a straight answer about whether residential is right for your situation, including if we think outpatient would work just as well.
What Role Does Your Prior Treatment History Play?
Prior treatment failure is one of the strongest qualifiers for inpatient rehab. If you’ve completed a 30-day outpatient programme and relapsed, attended AA without sustained sobriety, or detoxed at home and started drinking again within weeks, the next step is residential — not another round of the same level of care that didn’t hold. Doing the same thing harder isn’t a treatment plan.
This is where people get stuck in a loop. They’ve tried outpatient, it didn’t work, they feel like a failure, so they try outpatient again because the next step feels too big. Each failed attempt erodes confidence and, in the case of repeated detoxes, raises the medical stakes through kindling. The data on this is unambiguous: repeated unsupervised withdrawal episodes worsen subsequent withdrawals (Becker, Alcohol Health and Research World, 1998).
If this describes you, residential isn’t an escalation — it’s the appropriate level of care your previous attempts indicated you needed. Our guide to inpatient vs outpatient rehab covers when each level fits, and the complete guide to inpatient alcohol rehab walks through what 30–90 days residential actually looks like day-to-day. For the medical side of stopping, see our alcohol detox and withdrawal guide.
What About the Practical and Financial Side?
Inpatient rehab requires you to step away from work, family, and daily life for 28–90 days, and to pay for treatment that ranges from $5,000 to $30,000+ per month depending on the facility. Most international clients also need to budget for flights, visa or visa extension, medication, and personal expenses. The practical question isn’t usually “can I afford it” but “what does it cost me to not do it” — measured in another relapse, another hospital visit, or another year lost.
One Step Rehab charges ฿280,000/month (~$8,500 USD). That fee covers accommodation in a private room, three meals a day, the therapy programme, group sessions, intake assessment, routine progress checks with our visiting psychiatrist, and access to our activities and excursions. The fee does not include medication, airfares, visa fees, hospital visits, additional counselling beyond the programme, supplements, or personal items. Medication is billed separately — you pay for whatever the doctor prescribes during your stay. The full breakdown is on the pricing page.
| Tier | Monthly cost (USD) | Typical setting |
|---|---|---|
| Budget | $2,000–$5,000 | Shared rooms, lower staff ratios, regional facilities |
| Mid-range (One Step) | $6,000–$12,000 | Private rooms, structured programme, professional staff |
| Luxury | $25,000+ | Resort-style amenities, single-client suites, executive privacy |
Treatment length is the strongest predictor of outcome — longer stays consistently correlate with better recovery rates than shorter ones, regardless of facility tier (NIAAA Alcohol Treatment Navigator, 2024). A 28-day stay at a mid-range facility usually outperforms a 14-day stay at a luxury one. If finances force a trade-off between length and amenities, choose length.

How Does One Step Decide Who Qualifies?
Our admissions process screens for three things: severity of alcohol use, withdrawal risk, and suitability for the residential format. Severity and risk determine whether you start with on-site detox or with our partner hospital. Suitability covers whether the residential setting itself will help — most clients fit, but a few situations (active suicidal crisis, untreated psychosis, severe medical conditions requiring hospital care) need a different setting first.
What an intake conversation looks like:
- Drinking history — how much, for how long, daily pattern, prior periods of sobriety.
- Withdrawal history — prior detoxes, any seizures, DTs, or hospitalisations linked to stopping.
- Mental health — current or past diagnoses, medications, suicidal thoughts.
- Medical history — liver function, blood pressure, other conditions that affect detox safety.
- Home situation and treatment history — what you’ve tried before and why it didn’t hold.
Based on those answers, we either admit directly to One Step, recommend the partner hospital first with transfer to us once stabilised, or — occasionally — tell you another setting would serve you better and refer accordingly. The admissions process page walks through this in more detail, and the treatment schedule shows what daily life looks like once you arrive.
What we don’t do
We’re not a locked psychiatric facility. For active psychosis or an acute suicidal crisis, hospital admission comes first. We don’t accept under-18s. We’re a structured residential treatment programme, not a detox-only facility — and we’re not the cheapest or the most luxurious. We’re mid-range, focused on treatment quality.
Frequently Asked Questions
Common questions about qualifying for inpatient alcohol rehab.
Yes. Holding down a job doesn’t disqualify you from inpatient rehab — it just means the consequences haven’t surfaced yet. If you meet 4 or more DSM-5 criteria, drink daily, can’t sustain abstinence at home, or have prior failed detoxes, your work performance isn’t the right metric. Many of our clients are functional professionals.
There’s no universal threshold, but a useful rough guide: more than 8 standard drinks per day for several years usually means meaningful physical dependence and a real withdrawal risk. Total daily intake matters less than pattern and duration. Drinking 6 a day for 15 years is medically harder to stop than drinking 12 a day for 6 months.
No — and you shouldn’t. Most One Step clients arrive still drinking and detox under medical supervision on-site. Severe cases detox at our partner hospital first, then transfer for the rehab programme. Attempting to detox alone before admission is the opposite of what we recommend, especially if you have any of the withdrawal risk factors listed above.
For most diagnoses, no — depression, anxiety, PTSD, ADHD, and bipolar disorder in stable phases are well within what residential dual diagnosis treatment handles. Active psychosis, an acute suicidal crisis, or untreated severe bipolar mania need hospital-level psychiatric stabilisation first. We’ll tell you straight at intake which category you fall into.
That’s one of the clearest indicators for inpatient. A previous outpatient programme or detox that didn’t hold means the level of care wasn’t sufficient for your situation — not that you failed. Residential interrupts the cycle in a way outpatient can’t, particularly if home environment or co-occurring mental health was undermining the previous attempt.
Most clients stay 28 to 90 days. Twenty-eight days is the minimum to complete detox, stabilise, and build the foundations of the recovery programme. Sixty to ninety days produces meaningfully better outcomes — long enough for therapy gains to consolidate and aftercare planning to be realistic. We’ll tell you at intake what we think your situation needs.
Sometimes — international health insurance policies and some private domestic policies cover residential addiction treatment abroad. Coverage depends heavily on the policy and country. Our admissions team can help you check whether your insurer pays directly or reimburses, and what documentation they’ll need. Don’t assume either way without checking.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








