Key Takeaways
- Outpatient alcohol rehab works best for mild alcohol use disorder (2–3 DSM-5 criteria), where a person can keep their job, stay with family, and use the support network they already have.
- It is unsafe for severe withdrawal. Outpatient detox is contraindicated for anyone at risk of delirium tremens, seizures, or who has medical complications like cirrhosis or pancreatitis.
- Real cost savings. A 12-week outpatient programme typically costs a fraction of residential treatment — but only if you complete it. First-month dropout in outpatient substance abuse programmes is roughly 30%.
- The environment problem. Outpatient keeps you in the same home, social circle, and bar route that built the habit. For moderate-to-severe AUD, that’s often the variable that decides whether treatment sticks.
- Project MATCH showed something honest: well-run outpatient and residential programmes produce similar drinking outcomes for many people. The match between the person and the level of care matters more than the brand of therapy.
Outpatient alcohol rehab keeps your job, your family, and your costs intact — and for mild alcohol use disorder it works. But for moderate-to-severe AUD, staying in the environment that built the habit is usually the variable that decides whether the treatment sticks. The honest answer to “is outpatient enough?” is: it depends on how severe the drinking is, whether withdrawal is dangerous, and whether home is part of the problem (NIAAA, 2024).
What Is Outpatient Alcohol Rehab?
Outpatient alcohol rehab is structured treatment for alcohol use disorder that you attend during the day or evening while living at home. Sessions typically include individual counselling, group therapy, CBT, and sometimes medication management with naltrexone, acamprosate, or disulfiram. Hours range from one session a week to 20 hours across intensive outpatient programmes.
The American Society of Addiction Medicine (ASAM) groups outpatient care into Level 1 (under 9 hours of treatment a week) and Level 2 (intensive outpatient, 9–20 hours). Residential and inpatient care sits at Level 3 or above. Placement depends on six clinical dimensions — withdrawal risk, biomedical conditions, emotional or behavioural conditions, readiness to change, relapse potential, and the recovery environment at home (ASAM Criteria).
That last dimension — what your home environment actually looks like — is the one most people underestimate when they choose outpatient because it’s cheaper.

What Are the Real Benefits of Outpatient Alcohol Rehab?
The real benefits of outpatient alcohol rehab are practical: you keep your job, you stay with your family, you pay less, and you build recovery skills inside the life you actually live. For mild AUD with a stable home, evidence shows it can be as effective as residential treatment — and the support network you already have stays intact throughout.
Each benefit deserves an honest look, because each one has a flip side that matters depending on how severe the drinking is.
You keep your job and income
This is the single biggest reason people choose outpatient. Most programmes schedule sessions around work — early mornings, evenings, or one full day a week. You’re not explaining a 30-day absence to your boss. You’re not burning through paid leave or short-term disability. For self-employed clients or anyone whose income depends on showing up daily, this can be the deciding factor.
The flip side: if your job is part of the trigger (high-stress, drinking culture, long lunches with clients), going straight back to it every day during treatment can sabotage your recovery before the new skills set.
You stay with your family
You sleep at home. You see your kids. Your partner can be involved directly in family sessions. For parents who can’t be away for a month, this is non-negotiable. Family support is also one of the strongest predictors of long-term recovery, and outpatient lets you build it in real time rather than rebuilding it after a residential stay.
The flip side: if there’s an active drinker in the home, or unresolved conflict, or anyone who minimises your problem, you’re treating in the same environment that made you sick.
It costs less
This is the honest selling point most clinics avoid quoting. A standard 12-week intensive outpatient programme in the US runs roughly $3,000–$10,000. Residential treatment in the US runs $20,000–$60,000 for 30 days at the same tier. International residential options (including alcohol treatment in Thailand) sit between the two — typically $7,000–$15,000 a month, which still buys longer stays than US residential.
The flip side: cost only matters if you finish. First-month attrition in outpatient substance abuse programmes is roughly 30%, and drop-out before three months can exceed 50% (Walton et al., J Stud Alcohol, 1993). A cheaper programme you don’t complete costs more than an expensive one you do.
The evidence base is real — for the right cohort
Outpatient is not a budget compromise. For mild AUD with a stable environment, the research is clear: structured outpatient treatment produces durable change. A 24-month follow-up study of outpatient alcohol treatment found 58.2% of patients abstinent at follow-up, with an 84% programme completion rate during treatment (Soyka et al., Subst Abuse Treat Prev Policy, 2009). Project MATCH, the largest alcohol treatment trial ever run, found that three different outpatient therapies — CBT, motivational enhancement, and 12-step facilitation — produced broadly similar outcomes, with significant and sustained improvements from baseline through three years (Project MATCH Research Group, Alcohol Clin Exp Res, 1998).
The flip side: those positive numbers come from patients who were eligible for outpatient in the first place. People with severe AUD, unstable housing, active suicidal ideation, or risk of complicated withdrawal were screened out of those studies. The evidence base doesn’t automatically extend to them.

Where Does Outpatient Alcohol Rehab Fall Short?
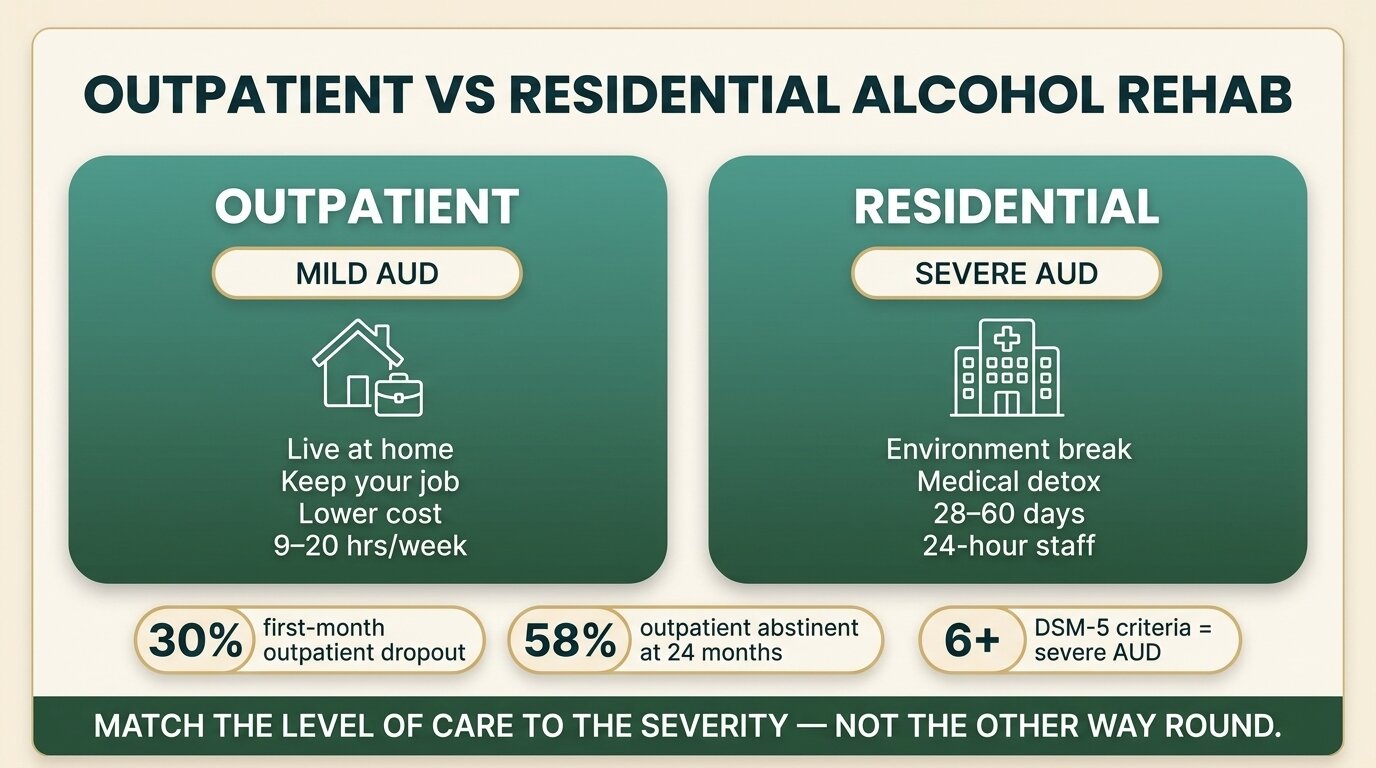
Outpatient alcohol rehab falls short for moderate-to-severe AUD in four predictable ways: it can’t safely manage severe withdrawal, it doesn’t break you out of the drinking environment, it leaves peer-pressure and access intact, and it relies on willpower that has already failed. For people who meet 6 or more DSM-5 criteria, residential treatment is usually the more honest recommendation.
| Factor | Outpatient suits you if… | Residential suits you if… |
|---|---|---|
| AUD severity | Mild (2–3 DSM-5 criteria) or moderate (4–5) with strong supports | Severe (6+ criteria), or moderate AUD with prior failed outpatient attempts |
| Withdrawal risk | Mild withdrawal — shaky hands, anxiety, mild sleep disruption | History of seizures, DTs, hallucinations, or heavy daily drinking (often 8+ units) |
| Home environment | Sober household, supportive partner/family, no active drinker present | Active drinker in the home, unresolved domestic conflict, or no stable housing |
| Co-occurring conditions | No active suicidal ideation, stable mental health, no major medical complications | Depression, trauma history, or medical conditions worsened by alcohol (cirrhosis, pancreatitis) |
| Previous attempts | First serious treatment attempt | Two or more failed outpatient attempts — pattern matters |
Severe withdrawal can’t be done outpatient
This is the medical line. Outpatient detox is contraindicated for anyone at risk of life-threatening withdrawal — delirium tremens, withdrawal seizures, hallucinations — or who has medical conditions like cirrhosis, pancreatitis, or gastrointestinal bleeding (Hayashida, Alcohol Health Res World, 1998). DTs kill roughly 1 in 20 people who experience them without medical treatment. Mild withdrawal — shakes, anxiety, trouble sleeping — can be tapered with benzodiazepines or gabapentin under outpatient supervision. Severe withdrawal needs a medical setting.
If you’ve been drinking 8 or more units a day for weeks, if you’ve had a withdrawal seizure before, or if your hands shake the morning after — you need a medical assessment before choosing any outpatient programme. The full picture of what happens during alcohol withdrawal is laid out in our guide to alcohol detox and withdrawal, and the side effects of alcohol detoxification covers the medical risks in detail.
The environment problem
You sleep in the same bed, drive the same route home, and stop at the same lights as the bar that knows your order. For someone with mild AUD and good supports, that’s manageable. For someone with moderate-to-severe AUD, it’s exhausting in a way the treatment hours can’t compensate for. The dopamine cues in your environment — physical places, people, smells, times of day — are doing the same work they were doing last week. You spend the sessions building skills and the rest of the week firefighting cues.
Residential treatment removes those cues entirely for 28–60 days. That isn’t a luxury, it’s a clinical mechanism. It gives the brain time to recalibrate without the environment constantly pulling it back. For deeper context on this trade-off, our post on inpatient vs outpatient rehab covers the specific clinical rationale, and who qualifies for inpatient alcohol rehab walks through the criteria.
Peer pressure and access stay intact
If your social life involves drinking — work events, sporting fixtures, weekly dinners with friends who all drink — outpatient does nothing to remove that pressure. You’re learning to refuse a drink while in the actual situation where you’d be drinking. Some people thrive on that exposure. Others relapse on it. The honest determinant is how severe the drinking became before you sought help.
It assumes willpower that has already failed
If you’re seeking treatment, you’ve probably tried to cut down before and not managed it. Outpatient asks you to do the same thing — control your drinking in your normal life — with more structure and skills. For mild AUD, that’s reasonable. For moderate-to-severe AUD, where the brain’s reward system has been recalibrated by years of heavy drinking, asking the same willpower to work again with a different toolkit often doesn’t.
The single most useful question I ask in an assessment is not “how much do you drink” but “what happens to you in the morning when you don’t.” If the answer is shaking hands, sweating, racing heart, or needing a drink to settle — outpatient detox is not safe. That person needs a medical setting first, and often a residential programme after. Choosing outpatient for severe alcohol use disorder is choosing the cheaper option that doesn’t work for that severity.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
How Do You Decide Between Outpatient and Residential?
The decision between outpatient and residential alcohol rehab comes down to three honest questions: how severe is your AUD on the DSM-5 scale, is your withdrawal medically dangerous, and is your home environment helping or hurting recovery. If you answer “severe”, “yes”, or “hurting” to any one of these, residential is usually the more appropriate level of care.
A useful clinical heuristic, drawn from the ASAM criteria: outpatient requires you to meet outpatient criteria on all six dimensions; residential only requires you to meet inpatient criteria on two of the six. That asymmetry exists because the stakes of getting it wrong are higher in one direction than the other.
Not sure which level of care fits your situation? Talk to our team — we’ll give you an honest assessment, including if we think outpatient near you would serve you better than flying out for residential.

How Does One Step Approach Alcohol Treatment?
One Step Rehab is a residential alcohol treatment programme in Chiang Mai, Thailand. We don’t run outpatient — for the clients who come to us, the environment break is the point. We handle standard alcohol detox on-site as part of the programme, and for severe withdrawal cases we detox you first at our partner hospital, which has intensive and intermediary intensive care units, before you transfer to us for the rehab programme.
Our structured treatment programme runs 28 or 60 days. The daily schedule includes individual counselling, group therapy, CBT and DBT, fitness, mindfulness, and weekend excursions. The fee is ฿280,000/month (~$8,500 USD). What that covers is on the pricing page. The fee does not include medication prescribed by the doctor, hospital visits, flights, visa fees, additional counselling sessions, or personal items — these are billed separately.
If outpatient is the right level of care for your situation, we’ll tell you that on the assessment call. We’re not the answer for someone who can use a community-based outpatient programme effectively. We’re the answer for people who need to step out of the environment that’s keeping them stuck.
Frequently Asked Questions
Common questions about outpatient alcohol rehab — when it works, when it doesn’t, and what to expect.
Yes — for mild alcohol use disorder with a stable home environment. Project MATCH and follow-up studies show outpatient produces durable change in well-screened patients. It is not effective, and often unsafe, for severe AUD or anyone at risk of complicated withdrawal. Effectiveness depends on matching the person to the right level of care, not on outpatient being “good” or “bad” as a category.
Mild alcohol withdrawal can be managed outpatient with a benzodiazepine or gabapentin taper. Severe withdrawal cannot. Outpatient detox is contraindicated if you have a history of seizures or delirium tremens, drink heavily every day, or have medical complications like cirrhosis, pancreatitis, or GI bleeding. Get a medical assessment before choosing any outpatient option.
In the US, a 12-week intensive outpatient programme typically costs $3,000–$10,000, depending on insurance coverage and provider. Standard outpatient (a few sessions a week) costs less. The number that matters more than the headline price is completion rate — a cheaper programme you don’t finish costs more than a longer one you do.
Yes — keeping your job is one of the main reasons people choose outpatient. Sessions are usually scheduled around work hours. The exception is if your work is itself a trigger — a drinking culture, high stress, long client lunches — in which case continuing without a break can undermine the treatment.
Standard outpatient is under 9 hours of treatment a week (ASAM Level 1) — usually one or two therapy sessions plus occasional group work. Intensive outpatient (IOP, ASAM Level 2) is 9–20 hours a week, often three evenings or full mornings, and is closer in structure to residential care minus the overnight stay.
Pattern matters. One failed outpatient attempt doesn’t necessarily mean outpatient was wrong — life circumstances, programme fit, or medication could have been the issue. Two or more failed outpatient attempts is usually a signal that residential is the more appropriate level of care, particularly if drinking has escalated between attempts.
Many outpatient programmes work alongside medication-assisted treatment using naltrexone, acamprosate, or disulfiram — the three FDA-approved medications for alcohol use disorder. Whether the medication is billed alongside the programme fee or separately depends on the provider. Ask before signing up.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn