Key Takeaways
- The first 72 hours of withdrawal carry the highest relapse risk. Symptoms peak in this window — anxiety, tremors, insomnia, intense cravings — and using again is the fastest way to make them stop. Most people who relapse during withdrawal do so before symptoms have peaked.
- Relapse during withdrawal is rarely about willpower. It’s a predictable response to acute physical discomfort plus easy access to the substance. Removing access is more reliable than relying on motivation.
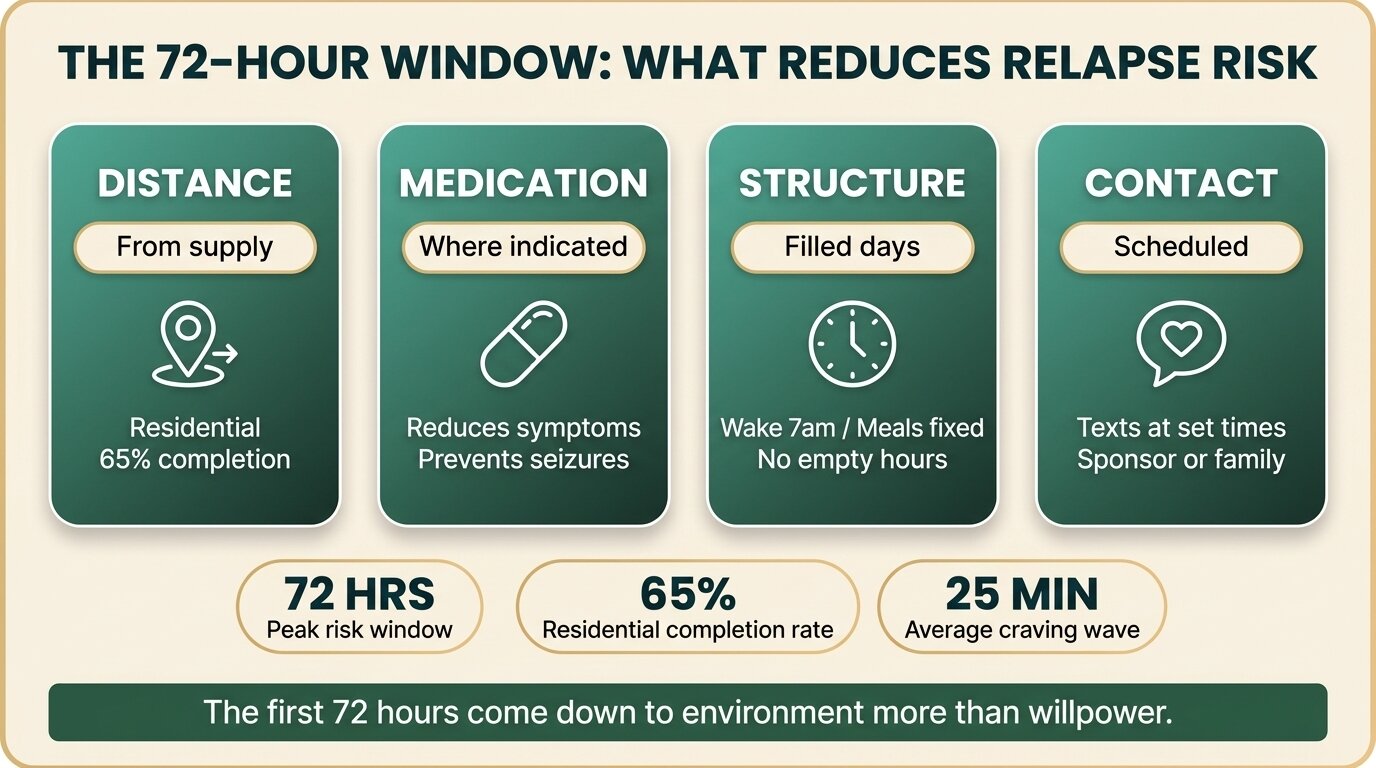
- The strongest protective factor is distance — physical distance from your usual supply, people, and places. This is why residential treatment outperforms outpatient detox for severe cases by roughly 25 percentage points on completion rates.
- Specific tactics that work: medication for withdrawal symptoms where indicated, regular sleep, hydration and electrolytes, scheduled check-ins, journaling craving spikes, and a structured day that doesn’t leave you alone with your thoughts.
- If residential isn’t possible, the next-best plan is a written 72-hour protocol: who you’ll be with, where you’ll sleep, who you call when cravings hit, and what medication you have access to. Verbal intentions don’t survive hour 36.
To reduce relapse risk during withdrawal, you need three things in place before symptoms peak: physical distance from your supply, medical support for the symptoms themselves, and a structured environment that doesn’t leave you alone with cravings. The first 72 hours carry the highest risk, because withdrawal symptoms peak within that window (Canver et al., StatPearls, 2024) and using the substance is the fastest way to make them stop.
This post is for someone trying to get through withdrawal without going back. It covers why that window is so dangerous, what actually protects you, and what to do if you can’t enter residential care. If you’re reading this for a family member who’s currently withdrawing, the practical 72-hour plan toward the end is the part you need.
Why Does Withdrawal Trigger Relapse?
Withdrawal triggers relapse because the substance is the fastest available solution to the symptoms it causes. Acute discomfort, anxiety, insomnia, and intense cravings all peak in the first 24–72 hours, and a single dose makes them stop within minutes. Without external structure to block that decision, the body’s drive to end discomfort wins.
The mechanism is straightforward. With chronic use, the brain adapts to the substance — alcohol upregulates glutamate and downregulates GABA, opioids downregulate the body’s natural pain control, stimulants deplete dopamine reserves. When the substance is removed, those adaptations leave the brain in a hyperexcitable, dysregulated state. That state produces real, physical symptoms: tremors and seizure risk for alcohol, bone pain and severe gastrointestinal distress for opioids, profound fatigue and anhedonia for stimulants. The substance is the only thing the brain knows can fix it quickly.
Sleep disturbance compounds the risk. Insomnia is one of the most consistent symptoms across every substance withdrawal, and research links poor sleep directly to higher craving intensity and relapse risk across alcohol, opioids, cocaine, nicotine, and sedatives (Brower & Perron, Medical Hypotheses, 2009). By night two or three, sleep-deprived judgement combines with peak symptom intensity — and that’s when most early relapses happen.
When Is Relapse Risk Highest During Withdrawal?
Relapse risk is highest between roughly 24 and 72 hours after the last use, when acute withdrawal symptoms reach peak intensity. For alcohol, symptoms begin within 6–12 hours and peak around 72. For short-acting opioids, peak distress is days 1–3. For long-acting substances like methadone or benzodiazepines, the peak shifts later but is also more prolonged.
The risk doesn’t end when acute symptoms subside. Post-acute withdrawal syndrome (PAWS) — a cluster of mood, sleep, and cognitive symptoms that can persist for weeks to months — is identified in clinical literature as a major contributor to later relapses (Zernig et al., Epidemiology and Psychiatric Sciences, 2025). Most people who get through the first 72 hours stop being in immediate danger of a same-day relapse, but they’re not safe — they’re in a different, longer phase of risk.
| Substance | Peak acute window | Highest-risk symptoms for relapse |
|---|---|---|
| Alcohol | 24–72 hours | Anxiety spike, tremors, insomnia, seizure risk |
| Short-acting opioids | 36–72 hours | Bone pain, GI distress, restlessness, intense cravings |
| Benzodiazepines | 2–7 days (varies with half-life) | Severe anxiety, insomnia, seizure risk |
| Stimulants (cocaine, meth) | 2–5 days | Crash fatigue, depression, anhedonia, sleep disruption |
| Nicotine | 2–3 days | Irritability, concentration loss, persistent craving |

What Protects You During Withdrawal?
The protective factors that reduce relapse risk during withdrawal are physical separation from supply, medical management of symptoms, structured time, and reliable human contact. None of these are about wanting it more — they’re about removing the option to use, dampening the symptoms that drive use, and filling the hours when cravings hit hardest.
Distance from supply, people, and places. The single most reliable protective factor is removing the option to use easily. Residential treatment outperforms outpatient detox on completion rates partly because of distance: in a U.S. comparison study, residential programmes had a 65% completion rate versus 52% for outpatient (Stahler et al., Addictive Behaviors, 2016). If you’re three minutes from your dealer or sharing a fridge with the alcohol, the distance from intention to use is too short to defend during peak symptoms.
Medical management of withdrawal symptoms. For alcohol and benzodiazepine withdrawal, benzodiazepines are the standard treatment — Cochrane’s review found a protective benefit against withdrawal seizures (Amato et al., Cochrane Database of Systematic Reviews, 2022). For opioid withdrawal, buprenorphine or methadone dramatically reduces craving and physical distress. Untreated withdrawal hurts more, and pain that has a chemical answer in your pocket is the highest-risk situation in addiction.
Structured days. Unstructured time is the enemy. A day that’s already filled — wake at 7, breakfast at 8, group at 9, exercise at 11, lunch at 12, individual session at 2, dinner at 6 — leaves fewer open hours for cravings to gather momentum. This is what residential programmes provide automatically and what outpatient clients have to construct themselves.
Reliable human contact. Cravings come in waves of 20–30 minutes. If there’s someone you can call or text who’ll talk you through one, the wave passes. If you’re alone scrolling your phone at 2 a.m. on night two, it doesn’t. This is the cheapest and most underrated protective factor, and it works for both residential and at-home recovery.
Going through withdrawal and trying to plan around relapse risk? Talk to our team — we’ll tell you honestly whether residential is the right call for your situation, or whether something less intensive would work.
What Specific Tactics Reduce Cravings During Withdrawal?
The tactics that reduce cravings during the first 72 hours of withdrawal are medication where appropriate, prioritising sleep, hydration with electrolytes, scheduled accountability check-ins, and writing cravings down instead of acting on them. Each one buys you minutes — and minutes is what you need, because individual craving waves typically last 20–30 minutes.
Medication-assisted withdrawal where indicated. For alcohol or benzodiazepine withdrawal, a doctor-prescribed tapering benzodiazepine protocol prevents seizures and dampens anxiety. For opioids, buprenorphine started in the right phase of withdrawal eliminates most physical symptoms within an hour. For stimulants, there’s no specific withdrawal medication, but sleep aids and antidepressants are sometimes used short-term. Self-detoxing from alcohol, benzos, or heavy opioid dependence at home is genuinely dangerous — don’t try it without medical input.
Sleep, even if it’s bad sleep. Sleep disturbance directly increases craving and relapse risk (Brower & Perron, Medical Hypotheses, 2009). Practical steps: dark room, no screens for an hour before bed, cool temperature, the same wake time every day. A doctor may prescribe a short course of a non-addictive sleep aid for the first week. Don’t drink alcohol “to sleep” — it produces the worst kind of sleep and resets the withdrawal clock.
Hydration and electrolytes. Withdrawal is a high-sweat, high-stress event for the body. Dehydration worsens headache, fatigue, and anxiety — symptoms that already feel like reasons to use. Aim for plain water plus an electrolyte source (oral rehydration salts, broths, or sports drinks if that’s what’s available). For alcohol withdrawal specifically, thiamine (vitamin B1) supplementation is standard medical practice to reduce neurological risk.
Journaling craving spikes. When a craving hits, write down the time, what triggered it, how strong it was on a 1–10 scale, and what you did. Two things happen. First, the act of writing slows the response by a few minutes — sometimes long enough for the wave to break. Second, after a week you have data: most cravings are weaker and shorter than they felt in the moment, and they’re patterned around specific triggers (boredom, evening, conflict). That data is useful later in therapy.
Accountability check-ins. Tell two people the exact times you’ll text or call them on day one, day two, day three. Not “I’ll reach out if I need to” — “I’ll text you at 9 a.m., 3 p.m., and 9 p.m. for the next three days.” Scheduled contact takes willingness out of the equation. Sponsors, family members, and treatment programme alumni are the most reliable. Friends who still use are not — even well-meaning ones.
What we see again and again is that the first 72 hours come down to environment more than character. Clients who relapse on day two almost never lacked the desire to stop — they were just alone, in their own home, with their phone and their dealer’s number and an hour to fill at 11 p.m. The protective factor isn’t motivation. It’s removing the option.
Alastair MordeyProgramme Director, One Step Rehab

Is Residential Treatment Necessary to Get Through Withdrawal?
Residential treatment isn’t always necessary, but it’s the highest-protection option — particularly for people withdrawing from alcohol, benzodiazepines, or opioids, or anyone who has relapsed during an at-home detox before. Residential provides distance, structured days, medical oversight, and on-site staff support automatically. At home, you have to engineer all of that yourself, while sick.
NIDA’s principles of effective treatment hold that treatment lasting fewer than 90 days is of limited effectiveness, and that longer durations consistently produce better outcomes (NIDA, Principles of Drug Addiction Treatment, 2018). The first 72 hours are the foundation that buys you the chance to do the rest. Detoxing successfully at home and then returning to a normal routine the next day is what produces the “I detoxed five times” pattern.
That said, if residential isn’t accessible, what you build at home matters. The next section is the practical version of that plan.
What Should a 72-Hour Withdrawal Plan Look Like If You’re Not in Residential Care?
A workable 72-hour withdrawal plan at home has four written elements: a medical contact, a location plan, a daily structure, and a craving-response protocol. Verbal intentions don’t survive hour 36. Whatever you decide before symptoms peak, write it down, share it with one other person, and follow it mechanically.
- Medical contact, named in advance. A GP, an addiction clinic phone line, or — for severe alcohol or benzo withdrawal — an emergency department you’re prepared to go to. Withdrawal from alcohol, benzodiazepines, or heavy opioid use can be medically dangerous. If you’re shaking badly, seeing or hearing things that aren’t there, or feeling like you might have a seizure, that’s an emergency, not a “should I bother someone?” call.
- Location plan. Where are you sleeping each of the three nights, and who’s there? Your own home with no one else present is the hardest version. A friend or family member’s house, with all substances removed from the premises, is significantly safer. Some people use a hotel for the first two nights to break the physical association with their usual using environment. Whatever the plan, decide before day one.
- Daily structure. Wake time, three meals, two scheduled phone calls, one walk, one shower at a fixed time. The schedule doesn’t have to be impressive — it has to be specific. “I’ll see how I feel” is not a schedule; it’s the gap that cravings fill.
- Craving-response protocol. A specific sequence for when a craving hits: drink a glass of water, set a 20-minute timer, text your contact, write down the trigger, do one physical task (shower, walk, dishes). The point is to occupy the 20–30 minutes until the wave breaks. The exact tasks matter less than having them pre-decided so you don’t have to think them up while distressed.

How Does One Step Approach Withdrawal and Early Relapse Risk?
One Step runs detox and rehab as a single continuous programme. Most clients detox on-site at our residential facility in Chiang Mai, with medical check-ins, medication where appropriate, and a gradual transition into the full therapy schedule as symptoms subside. For severe alcohol, benzodiazepine, or opioid dependence requiring intensive monitoring, we detox first at our partner hospital — which has intensive and intermediary intensive care units — then you transfer to One Step for the rehab programme.
The operational details that matter for the first 72 hours:
- Distance. The facility is in Chiang Mai, Thailand. Wherever you usually use is somewhere else. This is the highest-impact protective factor we provide and the one that’s hardest to replicate at home.
- Medical oversight during detox. Our visiting doctor manages medication for withdrawal symptoms — tapering benzodiazepines for alcohol or benzo withdrawal, opioid replacement protocols where indicated, sleep aids, anti-nausea medication, hydration support. Medication that’s prescribed is billed separately from the programme fee.
- Structured days from day one. Even during the detox phase, you have a schedule — meals, light exercise, one-to-one check-ins with staff, gradual reintroduction of group sessions as you stabilise. The day fills itself.
- Same-team continuity. The staff who get you through withdrawal are the same ones running your therapy programme. There’s no handover, no gap, no second admission.
- Programme fee. ฿280,000/month (~$8,500 USD). That covers accommodation, on-site therapy, group sessions, intake assessment, and routine medical check-ins. It does not cover medication, the partner hospital stay if needed for severe detox, flights, visas, or personal items.
Most clients stay 28–60 days. The first three to seven days are detox-focused; the rest is the actual treatment work. For more on what the residential day looks like, see our treatment schedule, our detox programme, and our pricing page for the full inclusions list. For context on residential versus outpatient outcomes generally, our post on why residential treatment works covers the comparison in detail. If you want to understand what alcohol withdrawal actually involves, our alcohol detox and withdrawal post goes through the timeline. And for the longer-term picture, our piece on the 10 most common relapse triggers covers what happens after the acute phase passes.
If you or someone you love is struggling with substance dependence, explore how a professional drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions about reducing relapse risk during the withdrawal window.
The highest immediate relapse risk is the first 72 hours, when acute withdrawal symptoms peak. After that, the risk shifts into a longer, lower-intensity phase tied to post-acute withdrawal symptoms — mood disturbance, sleep problems, intermittent cravings — which can persist for weeks to months and account for a large share of later relapses.
For mild dependence on substances like cannabis or nicotine, yes — though it’s still harder than people expect. For alcohol, benzodiazepines, or heavy opioid dependence, no. Withdrawal from those substances can produce seizures, severe dehydration, or cardiac events. At minimum, talk to a GP or addiction service before attempting it, and have an emergency contact ready.
Three reasons. Insomnia is one of the most common withdrawal symptoms, so you’re awake when you’d normally be asleep. Sleep deprivation impairs the judgement you’d use to ride a craving out. And night is when most people are alone, unscheduled, and bored — the conditions that let a craving build instead of pass.
Remove physical access to the substance and don’t be alone. Those two things, in combination, do more than any single tactic. If your supply is in the next room and you’re by yourself at 2 a.m. on night two, no amount of motivation will reliably hold. Distance plus presence is the foundation.
No. Relapse rates for substance use disorders are in the same range as relapse rates for other chronic conditions like hypertension and asthma. A relapse during the acute window usually points to a structural problem — too little distance from supply, too little symptom relief, too much unstructured time — not a personal failure. Most people who eventually recover relapse at least once along the way.
For heavy alcohol dependence with seizure history, severe benzodiazepine dependence, or opioid dependence with serious medical complications, we detox first at our partner hospital — which has intensive and intermediary intensive care units. Once medically stable, the client transfers to One Step for the full rehab programme. The two services run as a single coordinated process, not separate admissions.
No. The programme fee covers accommodation, therapy, group sessions, intake assessment, and routine medical check-ins. Any medication the doctor prescribes — tapering benzodiazepines for alcohol withdrawal, opioid replacement medication, sleep aids — is billed separately. Treat it like flights or visa fees: a clearly excluded personal cost.
Written by
Alastair Mordey
Alastair Mordey is one of the pioneers of drug and alcohol treatment globally and specifically in Asia. He has been an addiction’s professional for twenty years. He started his career as an expert in substance abuse w...
Learn more about Alastair
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn