Key Takeaways
- Yes, the entire point of outpatient rehab is to keep working — Intensive outpatient (IOP) runs about 9-12 hours a week, often evenings, designed around employment.
- Standard outpatient is lighter — 1-3 hours per week of individual plus group sessions. Partial hospitalisation (PHP) is 20-30 hours a week and behaves more like a part-time job.
- FMLA in the US, the Equality Act in the UK, and the Fair Work Act in Australia all give you a legal route to take treatment leave without disclosing addiction by name — but the protections aren’t automatic.
- Completion rates favour residential — In a national SAMHSA dataset, outpatient programs finished at 52%, residential at 65% (Stahler et al., Addict Behav, 2016). If your situation predicts you’ll be in the 48% who don’t finish, four weeks residential is often the shorter path back to work.
- One Step is residential, not outpatient — we don’t offer IOP. What we do offer: timing your stay around work commitments, employer leave letters, and 12 months of aftercare to handle the return-to-work transition.
Yes — outpatient rehab is specifically designed around keeping your job. Intensive outpatient programmes (IOP) typically run 9-12 hours per week, often clustered into evening or early-morning sessions so you can be at your desk during business hours (SAMHSA TIP 47, 2006). The harder question isn’t whether outpatient permits work — it does. The harder question is whether your specific situation, addiction severity, work schedule, and home environment, actually let outpatient succeed. For a large minority of people, it doesn’t, and pushing through anyway costs more job time, not less.
How Many Hours a Week Does Outpatient Rehab Actually Take?
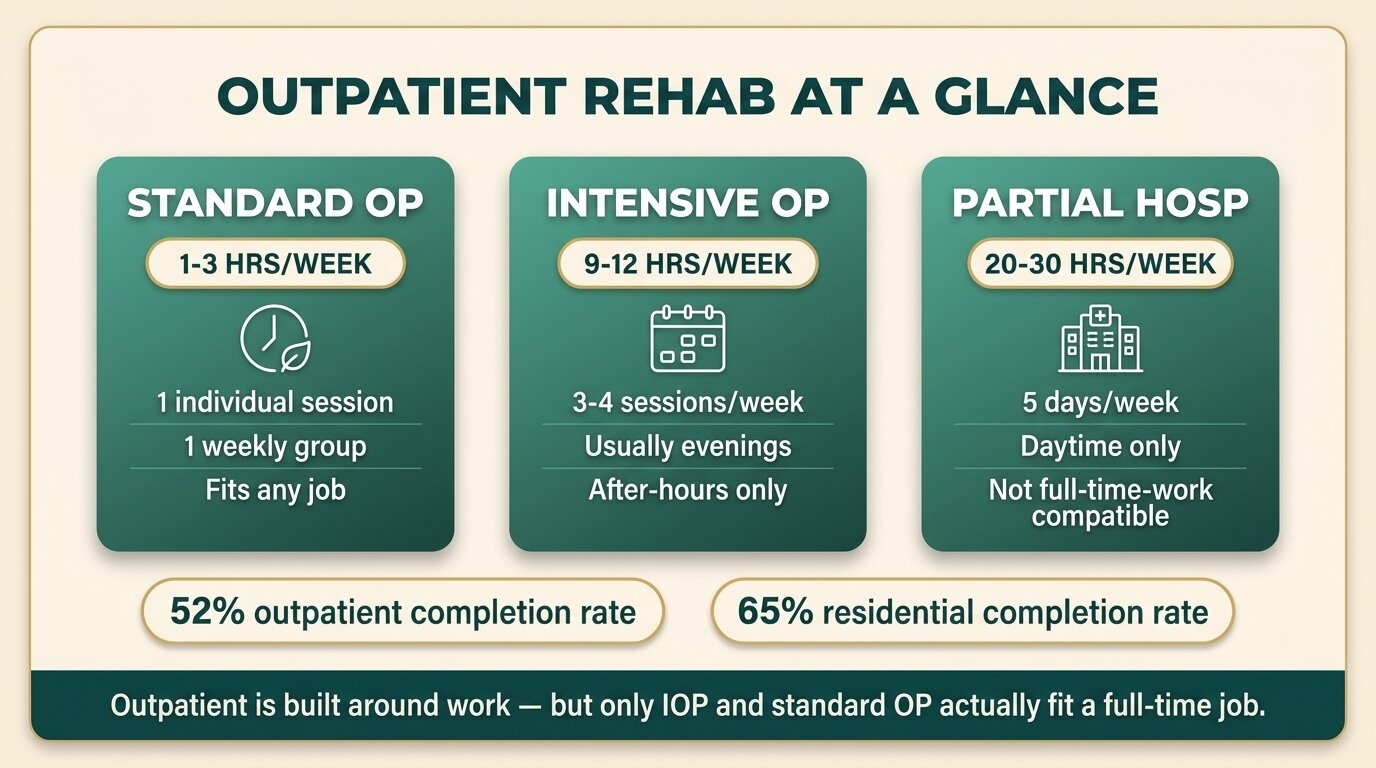
Outpatient rehab time commitment varies by level: standard outpatient is roughly 1-3 hours per week (one individual session plus one group), intensive outpatient (IOP) is 9-12 hours across three or four sessions, and partial hospitalisation (PHP) is 20-30 hours and behaves like a part-time job. Most IOPs schedule sessions in evenings or early mornings specifically so employed clients can attend without taking leave.
The American Society of Addiction Medicine (ASAM) sets the formal threshold: IOP is Level 2.1, defined as nine or more hours of structured programming per week (SAMHSA TIP 47, 2006). In practice, programmes cluster differently:
| Level | Hours per week | Typical schedule | Work impact |
|---|---|---|---|
| Standard outpatient (OP) | 1-3 hours | One individual session + one group, weekly | Minimal — fits around full-time work |
| Intensive outpatient (IOP) | 9-12 hours | 3-4 sessions/week, often 6pm-9pm | Significant after-hours commitment |
| Partial hospitalisation (PHP) | 20-30 hours | 5 days/week, daytime | Cannot be combined with full-time work |
The honest read: standard outpatient is compatible with most jobs without disclosure. IOP is compatible if your evenings are genuinely free and you can be in the same place at the same time three times a week for several months. PHP is not compatible with a full-time job, full stop — it’s the option people choose when they’ve taken medical leave but don’t need or want a residential stay.
What Legal Protection Do You Have If You Tell Your Employer?
If you work in the US, the Family and Medical Leave Act (FMLA) gives eligible employees up to 12 weeks of unpaid, job-protected leave per year for substance abuse treatment provided by a healthcare provider (US Department of Labor, FMLA Mental Health Guidance). UK employees are protected under the Equality Act 2010 if a co-occurring condition meets the disability threshold. Australian employees can take personal/carer’s leave under the Fair Work Act 2009.
The framing matters. None of these laws require you to disclose addiction by name. The legally protected category is almost always something broader — “serious health condition”, “medical treatment”, “personal illness”. A typical script for the HR conversation:
“I need to take medical leave for a health condition that requires treatment. My doctor has signed off on the leave. I’d prefer not to disclose specifics. Here is the medical certificate.”
What’s private and what’s not:
- Private: Diagnosis, the substance, the treatment facility name, specific medications.
- Not private (in most jurisdictions): The fact that you’re on medical leave, the rough duration, that a healthcare provider has authorised it.
- Often required by HR: A medical certificate or doctor’s letter — the letter does not need to specify “addiction” and a good treatment provider will write it without that word.
The Americans with Disabilities Act (ADA) protects employees with a history of substance use disorder who are not currently using illegal drugs. Active using is not protected. This is why the conversation with HR almost always happens after you’ve started or committed to treatment, not before — once you’re in treatment, you’re a person with a medical condition. Before, you’re a person with an active drug problem who may also be in breach of company policy.
The practical implication: you don’t have to tell your employer you’re “going to rehab”. You do typically need a medical certificate to access the legal protections. Treatment providers write these regularly. Ask before you go.
Does Outpatient Rehab Affect Job Performance?
Outpatient rehab almost always improves job performance once treatment takes hold — but the first 30 to 60 days are usually worse than baseline, not better. Sleep is disrupted, anxiety spikes, energy drops, and the brain’s reward system is recalibrating. People sometimes look more impaired in early recovery than they did while drinking, because the drinking was masking the underlying state.
The pattern matters because most people imagine starting outpatient and being instantly more reliable. The reality runs the other direction for the first month. That’s why employers who know about the treatment are often more useful than employers who don’t — they extend slack during the bad weeks instead of writing them up.
If you continue drinking or using while in outpatient, performance gets worse, not better. The combination of treatment fatigue (group three nights a week), poor sleep, lingering substance use, and the cognitive load of pretending nothing’s happening to colleagues is harder than just doing the job hungover.
The blunt version: outpatient works if you actually use it. Showing up to group while still drinking on the weekends doesn’t produce abstinence; it produces the appearance of treatment without the substance. Programme directors see this pattern constantly — and it’s the strongest single predictor of outpatient failure.
The biggest mistake we see in outpatient candidates is the assumption that going to group three nights a week is enough on its own. It isn’t. Outpatient rehab only works if everything else around it — the drinking partners, the bar after work, the bottle of wine with dinner — also changes. If those things can’t change while you’re still at work, outpatient is not the right call. A four-week residential stay is often shorter, cheaper, and more disruptive to addiction than a year of failed outpatient.
Alastair MordeyProgramme Director, One Step Rehab

When Does Outpatient Plus Work Fail?
Outpatient rehab combined with continued work fails most predictably when five conditions stack: moderate-to-severe addiction with active using at intake, no break from the home or social environment that fed the addiction, high-stress work with long hours, a peer-drinking workplace culture, and significant financial pressure. With three or more of these stacked, outpatient relapse rates climb sharply.
The Stahler study analysed the SAMHSA national treatment dataset and found outpatient programmes completed at 52% versus residential at 65% (Stahler et al., Addict Behav, 2016). Controlling for other variables, residential clients were nearly three times as likely to finish treatment as outpatient clients. The completion gap matters because completing the programme is one of the strongest predictors of one-year sobriety.
The honest read of the failure conditions:
| Risk factor | Why it predicts failure |
|---|---|
| Moderate-to-severe physical dependence | Daily withdrawal cycle pushes you back to using before therapy can take effect |
| No environmental break | Same triggers, same supply, same drinking partners daily |
| High-stress, long-hours job | No bandwidth left for therapy homework, sleep hygiene, or coping practice |
| Peer-drinking workplace | Friday drinks, client dinners, conference open bars — chronic exposure |
| Financial stress | Stress hormone load drives craving; therapy feels like a luxury you can’t afford |
| Previous failed outpatient attempts | Same approach producing same result; the structural problem hasn’t changed |
If three or more of these apply, the realistic question isn’t whether outpatient can squeeze into your work schedule — it’s whether you’ll still have the job in 12 months if you choose outpatient and it doesn’t hold. A relapse cycle of outpatient → drinking → emergency room → medical leave → restart, repeated two or three times, is more disruptive to a career than a single 28-day residential stay with proper return-to-work planning.
Not sure which level of care fits your situation? Talk to our team — we’ll give you a straight read on whether residential or outpatient is the better call for your case, even if the answer means going somewhere else.

When Does Residential Make More Sense Than Outpatient — Even If You’re Employed?
Residential treatment is the more efficient choice when addiction severity, environment, or work culture would make outpatient unlikely to hold. Four focused weeks of residential treatment plus a structured return-to-work, paired with months of remote aftercare, often disrupts a career less than a year of outpatient-attempts-and-restarts. Employed clients book residential more often than people assume, precisely because it’s the shorter path back to functional working life.
The decision often comes down to one question: can your home and social environment actually change while you’re in outpatient? If the answer is no — same flat, same drinking partner, same Friday client dinners — then outpatient is asking you to do the hardest psychological work in the hardest possible setting. Residential removes the environment for long enough to install new patterns. NIDA’s review of treatment research notes that participation in treatment for less than 90 days is of limited or no effectiveness (NIDA, Principles of Drug Addiction Treatment, 2018); residential gets you through the critical first month in conditions designed for it.
A 2006 study of employed adults completing residential treatment found 65% were retained by their original employer at 12-month follow-up, with measurable reductions in absenteeism and employment-problem days (Slaymaker & Owen, J Subst Abuse Treat, 2006). Residential plus return-to-work, in other words, is not the career-ender it’s often imagined to be.
Read our longer breakdown of inpatient vs outpatient rehab for a fuller comparison of the two pathways.
What Role Does One Step Rehab Play If You Want Outpatient?
One Step Rehab is a residential facility in Chiang Mai, not an outpatient programme — we don’t run IOP or PHP in any location. What we do offer employed clients: timing your residential stay around quieter work periods, employer leave letter packages that document medical leave without disclosing addiction, and 12-month structured aftercare so the return to work is supported rather than abrupt.
Our treatment programme runs 28-90 days residential, with most employed clients staying 28-42 days. The standard residential fee is approximately ฿280,000 per month (around $8,500 USD). The fee covers your room, three meals a day, group and individual therapy, fitness sessions, and group activities and excursions. Medication is billed separately — anything the doctor prescribes during your stay is your personal cost, the same way flights and visas are.
For employed clients specifically, our admissions team supports:
- Medical leave documentation: a healthcare-provider letter for FMLA, Equality Act, or Fair Work Act purposes — written without using the word “addiction” if you prefer.
- Time-zone-aware family video calls: so you can stay in contact with home and remain partially in touch with key work matters when that’s actually helpful.
- Discharge planning around your start-back date: we work backward from the day you need to be back at your desk and structure the final week of your stay around that.
- Aftercare check-ins: weekly during the first three months back at work, then monthly through the first year — this is where the return-to-work pressure actually shows up.
If outpatient is genuinely the right call for you, residential isn’t what you need and we’ll say so. The cases where we recommend residential over outpatient are concrete: moderate-to-severe physical dependence, repeated outpatient failures, an environment that can’t change, or a job culture that makes sobriety harder to maintain at home than at work. Anything less than that, outpatient near home is usually fine.
Why Are the First 30 Days the Hardest If You Try Outpatient While Working?
The first 30 days of outpatient treatment are the hardest because withdrawal symptoms, sleep disturbance, mood swings, and reduced concentration all peak in that window — exactly when you’re also trying to maintain professional performance. Many clients use accumulated leave or short medical leave for the first month, then return to work part-time. Outpatient does not pause the biology of early sobriety just because you have meetings.
For alcohol specifically, the NICE guideline recommends one 60-minute CBT session per week for 12 weeks following assisted withdrawal, plus a medication option such as acamprosate or naltrexone (NICE CG115, 2011). The 12-week schedule is built around recognising that the brain needs sustained intervention for at least the first three months — and the first month of those three is the brutal one.
Practical options for handling the early window while keeping the job:
- Take two to four weeks’ leave for the front of treatment, then return part-time for the rest.
- Schedule the start of treatment for a quieter business period — after year-end close, before peak project season, in the gap between rotations.
- Negotiate a phased return: 50% schedule for two weeks, 75% for two weeks, then full.
- Avoid the temptation to “just power through” the first 30 days while attending evening IOP three times a week. The combined load is what breaks people.
The narrower honest framing: outpatient that allows zero leave at any point is outpatient designed to fail. Even one or two weeks of clean rest at the front transforms the outcomes.
Frequently Asked Questions
Common questions about working through outpatient addiction treatment.
For standard outpatient (1-3 hours per week), usually yes — one evening session and one therapy slot fit around most jobs. For intensive outpatient at 9-12 hours per week, you can technically attend without formal leave if all sessions are evenings, but the first 30 days are hard enough that many clients take 1-2 weeks at the start anyway.
No — under FMLA in the US, the Equality Act in the UK, and the Fair Work Act in Australia, you can take medical leave with a healthcare-provider certificate without naming addiction as the condition. You may need to tell HR that you require medical leave, but specifics of diagnosis and treatment are private. A treatment provider can write the certificate without using the word “addiction”.
FMLA paperwork requires medical certification of a serious health condition but does not require you to specify the diagnosis. HR personnel handling the leave are legally required to keep that information confidential. Direct managers typically learn only that you are on approved medical leave, not the reason. Insurance claims through employer-sponsored plans are a more common disclosure route — those are governed by separate confidentiality rules.
Relapse during outpatient is common — it’s one of the reasons completion rates are lower than residential. Your outpatient team will usually intensify treatment first (more sessions, medication review, possible PHP step-up). If using continues, the typical next step is a residential admission. Your employer is generally not told about a relapse unless it directly affects your work or attendance.
Often yes, in calendar terms. A 28-day residential stay plus structured aftercare typically requires four to six weeks of leave. A year of outpatient with two relapses and emergency interventions can require more cumulative work disruption — and lowers the chance you keep the job at all. The right comparison is total disruption over 12 months, not single-episode duration.
Partial hospitalisation (20-30 hours per week) is not compatible with a full-time job. People who choose PHP have usually taken medical leave but want to sleep at home rather than enter residential. IOP (9-12 hours per week, evenings) is the typical “still working” choice. If a clinician recommends PHP and you can’t take the leave, residential for a shorter period is usually the more honest alternative than downgrading to IOP and hoping for the best.
No — One Step Rehab is residential only, based in Chiang Mai, Thailand. We don’t run IOP or PHP. For employed clients, we structure the residential stay around work commitments, provide employer leave letters, and offer 12 months of remote aftercare to support the return to work. If outpatient is the right call for your situation, we’ll say so and recommend local options.
Written by
Alastair Mordey
Alastair Mordey is one of the pioneers of drug and alcohol treatment globally and specifically in Asia. He has been an addiction’s professional for twenty years. He started his career as an expert in substance abuse w...
Learn more about Alastair
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn