
Key Takeaways
- “High-functioning” describes appearances, not biology. Brain, heart, and dental damage track use intensity and frequency — not whether you make it to your 9am meeting.
- The most reliable signal is a cluster of changes over weeks, not any single tell. A Friday afternoon drop in output, weight loss without a diet change, and partner-reported sleep disruption together mean more than any one of them alone.
- Workplace patterns to track: meetings cut short for “calls,” a sudden Friday productivity decline, unexplained cash withdrawals, weight loss without explanation, and bathroom breaks every 30–45 minutes during long sessions.
- Physical clusters to track: a persistent runny or blocked nose, frequent nosebleeds, jaw tension or grinding noises at night, receding gums, and weight that fluctuates with no diet change.
- The “I still hold it together” argument is the most common reason functional users delay treatment by years. Earlier intervention is the difference between stopping cocaine and recovering from a heart attack at 42.
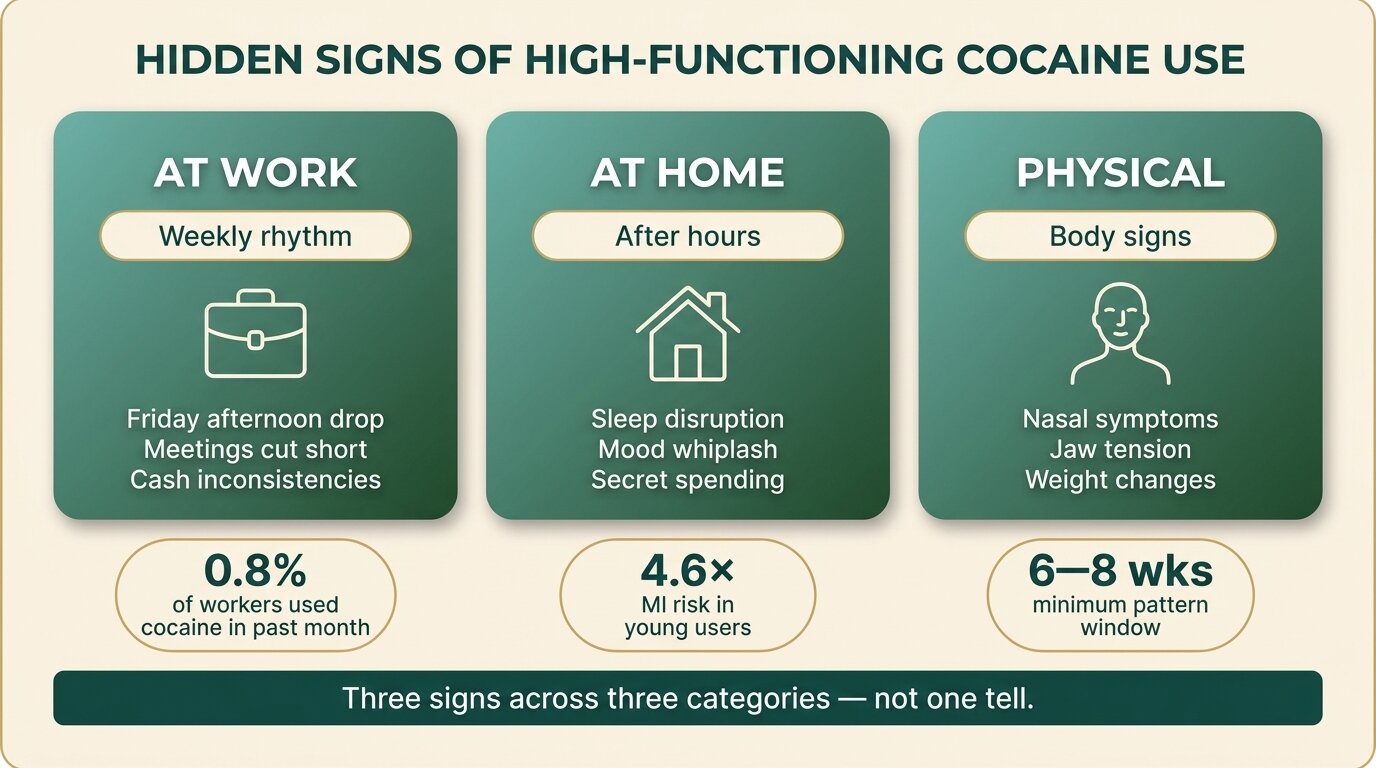
A “high-functioning” cocaine user is someone whose use hasn’t yet broken the visible parts of their life — the job, the relationship, the mortgage — but whose body, brain, and finances are accumulating damage in private. Studies of professional substance use put past-month cocaine use among 30–35 year-old workers at around 0.8%, with hotspots in food service, finance, sales, and the trades (Oh et al., Am J Ind Med, 2025). The signs are there. They just rarely show up in any single moment — which is why colleagues, partners, and the user themselves spend years missing a pattern that becomes obvious only in hindsight.
This post is a pattern checklist, not a diagnostic tool. You can’t “spot the signs from across the office” — anyone who tells you otherwise is selling something. What you can do is recognise a cluster of changes that line up over weeks or months, and use that pattern to start a conversation that might otherwise wait years.
Is “High-Functioning” a Real Category or Just Denial?
“High-functioning” is a description of what other people see, not a medical category. Someone can hold down a senior job and still meet every clinical criterion for cocaine use disorder. The phrase mostly serves as permission — a way for the user, the partner, and the employer to delay the conversation. The biology doesn’t care about your LinkedIn profile.
Cardiovascular damage and cognitive impairment track use intensity, not visible chaos. A review of cocaine’s cardiovascular effects found younger adults with more than 10 lifetime uses had roughly 4.6 times the risk of acute myocardial infarction compared to non-users — and that risk applies whether the user is sleeping on a sofa or running a sales team (Kim & Park, Int J Mol Sci, 2019). The brain shows similar patterns: chronic cocaine users score worse on attention, working memory, and inhibition tasks than controls, with the deficits proportional to use, not to whether the user “looks fine” (Vonmoos et al., Neuropsychopharmacology, 2014).
The good news in that same Vonmoos paper: cognitive function partially recovers with sustained abstinence. The bad news: by the time most functional users seek help, they’ve often been using for five to ten years.
What Are the Hidden Signs of Cocaine Use at Work?
Workplace signs of high-functioning cocaine use show up as a pattern of small inconsistencies: bursts of unusual confidence followed by withdrawal, meetings cut short for “urgent calls,” frequent bathroom breaks during long sessions, a sharp Friday afternoon decline in output, and weight loss without an explanation. Any one is forgettable. The cluster, repeated weekly, is not.
The pattern that distinguishes cocaine use from general stress or burnout is the rhythm. Cocaine has a short subjective high — typically 30 to 60 minutes for powder, less for crack — followed by a crash. In an office context, that produces a characteristic shape: animated, fast-talking, ideas-flowing in the first part of an extended session; quiet, irritable, or “stepped out” by the end of it. Wednesday afternoons and Friday afternoons are the most visible because Tuesday and Thursday nights are common use nights.
| Pattern | Stress or burnout | Cocaine use rhythm |
|---|---|---|
| Mood | Flat, low, consistent | Cycles within a week: animated, then withdrawn |
| Productivity | Gradual decline | Spikes on use days, drops 24–48 hours after |
| Meetings | Disengaged, distracted | Stepped out for “calls”, returns more talkative |
| Friday afternoons | Same as Monday | Notably quieter, leaves early, “tired” |
| Weight | Stable or slight gain | Loss without diet change; gain on time off |
| Spending | Reduced | Cash withdrawals on Thu/Fri, gaps in expense reports |
Finance is often the most concrete signal. Powder cocaine in the UK and Europe runs roughly £80–£120 per gram; in Australia and parts of Asia, two to three times that. A two-gram weekend habit can run £8,000–£12,000 a year — money that has to come from somewhere. Look for unusual cash withdrawals, vague expense entries, a partner asking why the joint account is empty, or a colleague who suddenly can’t cover a round of drinks at month-end.

What Cocaine Use Signs Show Up at Home?
At home, the signs cluster around sleep, mood whiplash, and secrecy. Partners often report the user staying up “working” until 2am, then crashing on weekends; mood swings that don’t track external events; bathroom doors locked for unusual lengths of time; and a creeping pattern of financial conversations that don’t add up. The home pattern is usually more vivid than the work pattern because the user isn’t performing.
Sleep is the most reliable early signal. Stimulant use disrupts sleep architecture for hours after the subjective high ends, and chronic users routinely report being awake at 3am scrolling, working, or “thinking.” Partners often describe sleeping alone for parts of the night, finding the user on the sofa in the morning, or noticing the same pattern on the same nights of the week.
The mood pattern is the second clearest. Cocaine produces a short euphoria, then irritability, anxiety, and a flat or low mood as dopamine levels drop. A partner watching this from the outside sees what looks like temperament whiplash — charm and animation one evening, withdrawn or snappy the next morning — without a clear external cause. Domestic friction tends to escalate around use days and weekends because that’s when the crash and the user are in the same room.
Secret spending is the third. Cash disappearing in £100 or £200 increments without an explanation, new accounts the partner doesn’t know about, withdrawn credit applications, or a sudden interest in “splitting the bills differently” are all worth taking seriously when they show up alongside the sleep and mood patterns.

What Are the Physical Signs of Cocaine Use to Watch For?
Physical signs of cocaine use include a persistent runny or blocked nose, frequent nosebleeds, white residue on facial tissues, a hoarse voice from post-nasal drip, weight loss without a diet change, jaw tension or audible teeth grinding, and gum recession visible at the dentist. The nasal symptoms are the most specific; the others overlap with stress and overwork, which is why the cluster matters more than any single sign.
Snorted cocaine damages the nasal lining through repeated vasoconstriction and direct irritation. The early signs are a constantly blocked or runny nose, a hoarse voice from drip down the throat, and a habit of sniffing or clearing the throat that wasn’t there a year ago. Over months and years, the same mechanism can erode the cartilage of the septum, producing nosebleeds, a whistling sound on inhale, and in advanced cases perforation of the septum or palate (Brand et al., Br Dent J, 2008).
Dental and jaw signs come from two directions. Cocaine’s vasoconstrictive effect on the gum tissue accelerates gum recession and gingival lesions, often picked up first by a dentist before either partner or user has named what’s happening. Separately, cocaine and other stimulants produce jaw clenching and grinding during the high — the muscles around the jaw stay tense for hours — which leads to morning jaw soreness, audible grinding at night, and worn tooth surfaces over time.
Weight changes are common but easier to miss because they go in two directions. During active use, body composition shifts toward lower fat mass, often without a corresponding drop in appetite — chronic users frequently report normal or elevated eating while staying lean (Billing & Ersche, Am J Drug Alcohol Abuse, 2015). Two to four weeks into abstinence, that pattern reverses sharply: a person who looked lean during their use years can put on 5–10 kg in their first months of recovery. Sudden weight gain in someone “who’s been doing well lately” is sometimes a recovery signal, not a relapse one.
Recognising the pattern in someone you care about? Talk to our team — we’ll tell you what we’d actually do in your position, without making you commit to anything.
How Can a Colleague or Partner Use This as a Checklist?
Treat the checklist as a pattern over weeks, not a single observation. Look for at least three signs from different categories — work rhythm, home behaviour, physical changes, financial inconsistency — that line up over six to eight weeks. A single dropped meeting or one bad nosebleed proves nothing. Three patterns reinforcing each other across categories is the signal worth acting on.
| Observer | Patterns most likely to be visible | Patterns rarely visible |
|---|---|---|
| Colleague | Friday-afternoon drop in output, frequent calls/breaks, weight loss, expense or cash inconsistencies | Sleep disruption, mood at home, dental changes |
| Partner or housemate | Sleep disruption on use nights, mood whiplash, locked bathroom time, cash going missing, weekend crash | Work rhythm, expense patterns |
| Dentist or GP | Gum recession, jaw wear, nasal lining damage, elevated resting heart rate or blood pressure | Behaviour, finances |
| The user themselves | Everything — but the “I’m fine, I’m still functioning” filter is almost always on | Honest accounting of frequency and spend |
If you’re the partner or colleague, the conversation you have isn’t a diagnosis. It’s a specific, observable description: “I’ve noticed you’ve been sleeping on the sofa on Wednesdays and Fridays for two months. I’ve noticed you stepped out of three meetings this week. I’m not accusing you — I’m worried, and I want to ask directly.” That is harder to deflect than “I’m worried about you,” because it forces the conversation onto pattern, not interpretation.
The clients I see at the residential phase are almost never the people whose lives have visibly fallen apart. They’re the ones whose lives still look intact on paper — partner, mortgage, job — but who have privately known for two or three years that the cocaine is running them, not the other way around. The “I still hold it together” argument is the single most common reason people delay treatment by years rather than months. By the time the visible part breaks, the cardiovascular and cognitive damage is already in the body.
David KaffSenior Therapist, One Step Rehab

When Should a Functional User Actually Get Help?
The honest answer is: before the cluster of signs becomes a cluster anyone else can see. The functional user’s window is the period when they can still take 30 days off work without a crisis, still negotiate residential treatment as planned leave rather than emergency leave, and still recover cognitive function without permanent loss. That window narrows every year of continued use.
The clinical markers worth taking seriously are: weekly or more-frequent use for more than 12 months; failed self-imposed limits (“just weekends,” “just at parties”) more than twice; any chest pain, palpitations, or panic episodes during or after use; nosebleeds that have started in the last year; and partner or family members raising concerns more than once. Any two of those, in our experience, is a clear “now, not in six months” signal.
The cognitive evidence is the strongest case for moving sooner. Vonmoos and colleagues found that cocaine users who stopped showed recovery toward control-group cognitive performance over a year — but users with earlier onset, in their late teens and early twenties, showed hampered recovery in working memory specifically. The longer the use, the longer the recovery takes, and some functions don’t fully return.
How Does One Step Treat Functional Cocaine Users?
One Step Rehab is a residential treatment programme in Chiang Mai, Thailand, designed around 28- to 60-day stays. For functional cocaine users — clients who arrive with their job, relationship, and finances still intact — we structure the programme around three things: physical recovery (sleep, cardiovascular, nutrition), the therapy work that addresses the use pattern itself, and a return-to-work plan that doesn’t burn the life they came in with.
A typical day starts at 7am with morning meditation or movement, breakfast at 8, group therapy 9–11, individual sessions or specialist groups in the afternoon, and structured evenings. The programme uses CBT and DBT as its primary therapeutic spine — we cover the differences in detail in our post on CBT and DBT for addiction — alongside trauma-informed work, group process, and a 12-step track for clients who want it. Outdoor therapy (treks, kayaking, temple visits) and a strict no-phones-first-week rule are deliberate.
Cocaine detox is handled on-site. Unlike alcohol or benzodiazepines, cocaine withdrawal is not medically dangerous — it’s miserable, but it doesn’t require ICU-level monitoring. Most functional users find the first five to ten days are dominated by exhaustion, low mood, and sleep that doesn’t yet feel normal. Our role at that stage is structure, food, sleep hygiene, and keeping clients engaged with the programme so they don’t decide on day four that they were “fine all along” and leave.
Pricing is ฿280,000/month (approximately $8,500 USD), which covers accommodation, all meals, group and individual therapy, the daily programme, an intake assessment with our visiting psychiatrist, routine progress checks, and the outdoor activities. Medication, if prescribed, is billed separately — like flights, visas, hospital visits, and personal items. The full pricing page is at /pricing/; we recommend reading the “fee does not include” list before deciding.
For more on what cocaine treatment specifically involves, see our cocaine rehab programme page, and our deeper post on the role of therapy in cocaine addiction recovery. If you’re trying to work out whether you’re crossing from heavy use into dependence, the post on cocaine abuse vs cocaine dependence is the most direct read. Functional users who also drink heavily should read our post on cocaethylene — the third compound your liver creates when alcohol and cocaine are both in your system — because that’s where the cardiovascular risk multiplies.
The honest limitation: residential treatment is a reset, not a guarantee. We expect clients to do the work, engage with group, and follow through with the aftercare plan we build with them in the last two weeks. The functional users who relapse usually do so because they treated the 28 days as a holiday rather than the start of the work.
If you or someone you love is struggling with substance dependence, explore how a structured drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions from partners, colleagues, and functional users themselves.
Yes. Cocaine use disorder is a clinical pattern of compulsive use despite consequences — it doesn’t require visible career collapse. Many functional users meet diagnostic criteria for years while still performing at work, which is why “I still have my job” is one of the most common reasons people delay treatment.
There isn’t one. Anyone claiming a single “tell” — bloodshot eyes, sniffing, restlessness — is overstating. The reliable signal is a cluster of changes (sleep, mood, finances, nasal symptoms, weekly rhythm) that line up across categories over six to eight weeks.
Lower than daily use, yes — but not low. The cardiovascular risks (heart attack, arrhythmia, stroke) are dose-dependent, but spikes in blood pressure during a binge can trigger an acute event in a single session. Each weekend of use carries its own risk of an acute cardiac event, regardless of how “controlled” the schedule looks.
Lead with specific observed patterns, not interpretations. “I’ve noticed you’ve been on the sofa on Wednesday and Friday nights for two months, and you’ve left three meetings this week” is harder to deflect than “I’m worried about you.” Avoid the words “addict” or “addicted” in the first conversation — they almost always shut it down.
Partially, and faster than most people expect. Vonmoos and colleagues found cocaine users who stopped recovered toward control-group cognitive performance over a year, with attention and inhibition improving most. People who started in their late teens or early twenties showed slower recovery, particularly in working memory.
For cocaine alone, no. Cocaine withdrawal is uncomfortable — exhaustion, low mood, disrupted sleep, food cravings — but it’s not medically dangerous. We handle cocaine detox on-site at One Step. Hospital detox is only relevant for severe alcohol, benzodiazepine, or opioid withdrawal, which carries seizure or cardiac risk.
28 days is the floor, 60 is what we recommend for established patterns. The first two weeks are largely physical and emotional reset. The deeper therapy work, group integration, and aftercare planning happen in weeks three to eight. Shorter stays do happen but rarely produce lasting change in users with years of established use.
Written by
David Kaff
David Kaff is an Addictions Counselor with over a decade of experience working in both harm reduction and residential treatment settings in Australia and Thailand. He has worked across frontline services, 12-step based r...
Learn more about David
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn








