
Key Takeaways
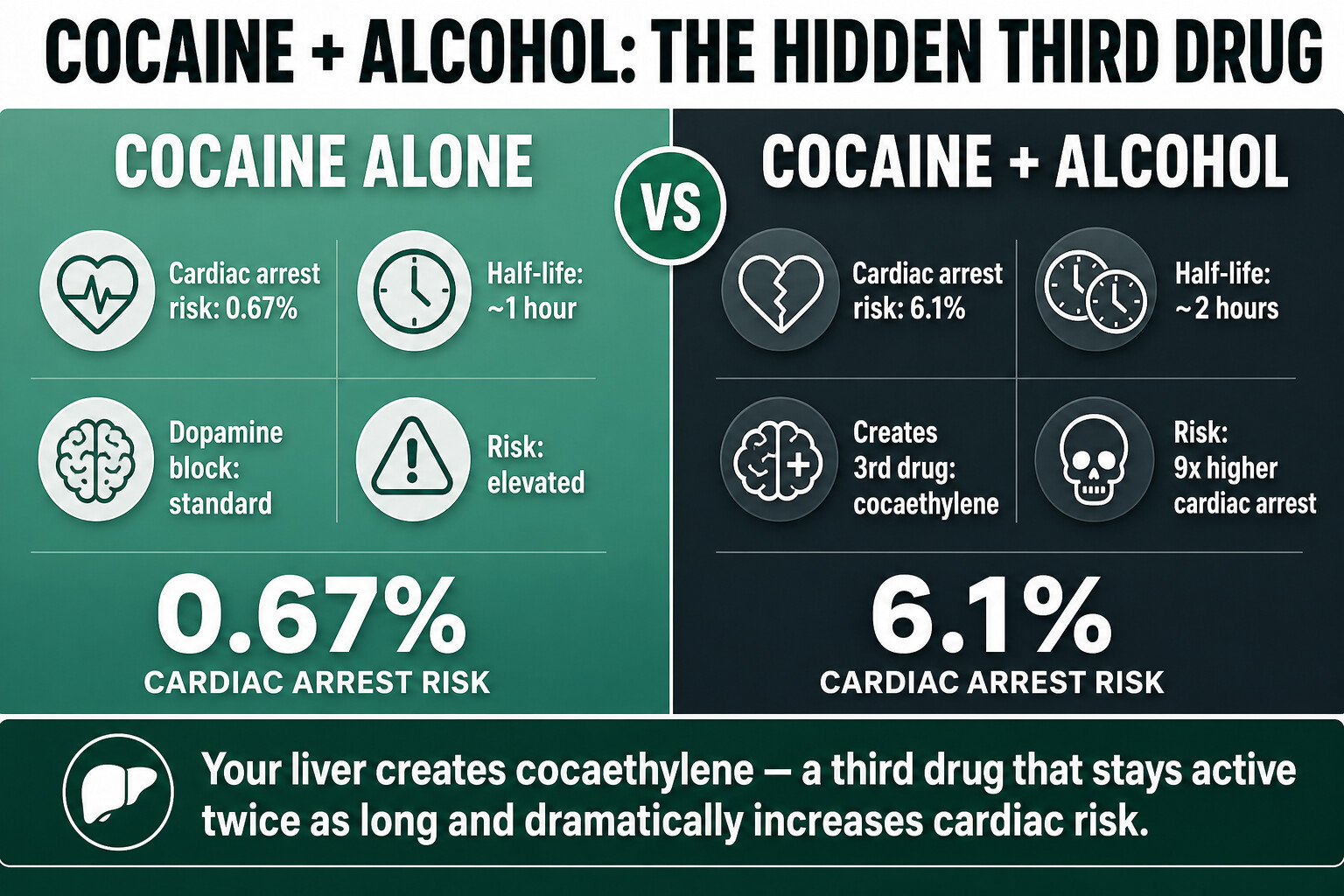
- When you use cocaine and drink alcohol at the same time, your liver creates a third substance called cocaethylene. It’s not just cocaine plus alcohol — it’s a new drug that your body produces on its own, and it’s more dangerous than either substance alone.
- Cocaethylene stays active in your body roughly twice as long as cocaine (about 2 hours vs 1 hour), extending the window for cardiac events, seizures, and overdose. The longer high is exactly why the combination feels appealing — and exactly why it kills people.
- Emergency room data shows that people with cocaethylene in their system are 9 times more likely to experience cardiac arrest than those who used cocaine alone (6.1% vs 0.67%).
- At least 62% of people who use cocaine regularly also drink alcohol — many without knowing their liver is manufacturing a third drug every time they do it.
- Treating cocaine-and-alcohol addiction together is essential. Addressing one while ignoring the other leads to relapse. At One Step, both substances are treated within the same residential programme from day one.
Mixing cocaine and alcohol doesn’t just add two drugs together — it creates a third one. When both substances are in your system at the same time, your liver produces cocaethylene, a unique metabolite that stays in your body longer than cocaine and significantly increases the risk of cardiac arrest, seizures, and sudden death (NIDA, 2024). Most people who combine these substances have no idea this is happening inside their body.
This isn’t a rare combination. Alcohol is involved in roughly a third of all cocaine-related emergency department visits in the United States — over 170,000 cases per year (Botelho et al., Acad Emerg Med, 2023). This post explains what cocaethylene actually does, why the combination is far more dangerous than people realise, and what treatment for co-occurring cocaine and alcohol addiction actually looks like.
What Is Cocaethylene and How Does It Form?
Cocaethylene is a pharmacologically active substance created in the liver when cocaine and alcohol are present in the body at the same time. The liver converts cocaine into cocaethylene through a chemical reaction with ethanol, producing a new compound that acts on the brain’s dopamine system with similar strength to cocaine itself — but stays active for roughly twice as long (Jones, J Anal Toxicol, 2019).
Here’s what matters in plain terms: your liver is designed to break down toxins. When you give it cocaine and alcohol at the same time, instead of breaking cocaine down safely, it produces a third drug. You didn’t take this drug. You didn’t buy it. Your body manufactured it from two substances you thought you were managing.
The amount of cocaethylene produced depends on how much cocaine and alcohol you consumed, the order you took them in, and your individual liver function. Drinking alcohol before using cocaine tends to produce more cocaethylene because the alcohol is already being processed when the cocaine arrives (Jones, J Anal Toxicol, 2019).
| Factor | Cocaine alone | Cocaethylene (cocaine + alcohol) |
|---|---|---|
| How it enters your body | Snorted, smoked, or injected | Created by your liver when cocaine and alcohol are both present |
| Half-life | ~1 hour | ~2 hours |
| Effect on dopamine | Blocks dopamine reuptake (produces high) | Equally effective at blocking dopamine reuptake |
| Cardiac risk | Elevated | Significantly higher — 9x cardiac arrest rate in ER data |
| Detectable in blood | ~6 hours after use | Several hours longer than cocaine |
Why Is Mixing Cocaine and Alcohol So Dangerous?
The combination of cocaine and alcohol is more dangerous than either substance alone because cocaethylene extends the duration of cardiac stress, blocks the heart’s sodium channels more potently than cocaine, and accumulates with repeated dosing over a session. The result: a significantly higher risk of cardiac arrest, seizures, stroke, and sudden death.
The numbers from emergency departments tell the story clearly. In a study of 199 patients presenting with acute drug overdose, cardiac arrest occurred in 6.1% of patients who had cocaethylene in their system, compared to 0.67% of those with cocaine alone. That’s roughly a ninefold increase in cardiac arrest risk from a single additional variable — alcohol (Botelho et al., Acad Emerg Med, 2023).
The danger comes from several overlapping mechanisms:
- Longer exposure window: Cocaine’s high wears off in about an hour. Cocaethylene keeps working for roughly two hours. That’s twice the window during which your heart, blood pressure, and brain are under chemical stress.
- Stronger cardiac sodium channel blockade: Cocaethylene blocks the heart’s sodium channels more potently than cocaine, disrupting the electrical signals that keep your heart beating in rhythm (Xu et al., J Pharmacol Exp Ther, 1994).
- Accumulation during binges: Because cocaethylene clears more slowly, each additional dose of cocaine (while still drinking) builds on the last. Over a night of repeated use, cocaethylene concentrations climb while cocaine levels fluctuate.
- Masking of alcohol impairment: Cocaine makes people feel more alert and less drunk than they actually are. This leads to drinking more, staying out longer, and taking more cocaine — all of which produces more cocaethylene.
“When someone presents to us having used cocaine and alcohol together, the risk profile is fundamentally different from either substance alone. The cardiac complications we see — irregular heartbeat, chest pain, dangerously elevated blood pressure — are more severe and more persistent. The combination isn’t additive. It’s synergistic.”
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
How Common Is Cocaine and Alcohol Use Together?
Using cocaine and alcohol together is not a fringe behaviour — it’s the norm among regular cocaine users. Research estimates that at least 62% of people who use cocaine regularly also use alcohol, and some studies put that figure as high as 90%. Ethanol co-ingestion is reported in 34% of cocaine-related emergency department visits across the United States (Botelho et al., Acad Emerg Med, 2023).
There are practical reasons the combination is so common. Alcohol is everywhere — at every bar, party, and social event where cocaine is typically used. But there’s also a pharmacological reason: cocaine makes the alcohol high feel sharper and more energised, while alcohol softens the jittery, anxious edge of cocaine. Users report the combination feels better than either substance alone. That’s not a coincidence — it’s because cocaethylene is producing its own dopamine surge on top of what cocaine is already doing (Hearn et al., Life Sci, 1991).
The problem: this reinforcing loop makes the combination extremely habit-forming. Many people who come to us for cocaine treatment have never used cocaine without alcohol. The two substances become psychologically linked — the smell of a beer triggers a craving for cocaine, or a line of cocaine triggers the urge to drink. Treating one without the other almost never works.
What Are the Signs That Cocaine and Alcohol Use Has Become a Problem?
A cocaine and alcohol problem has crossed from recreational use into dependency when the pattern becomes predictable, the quantities escalate, and attempts to stop or reduce use fail. Warning signs include needing both substances to feel “right” on a night out, using cocaine specifically to drink more, experiencing withdrawal or crashes that disrupt daily life, and hiding the extent of use from others.
Specific red flags to watch for:
- You can’t do one without the other. Every drinking session ends with cocaine. Every cocaine session requires alcohol to take the edge off.
- Quantities have increased. What started as a line or two has become half a gram, then a gram, then more — and the bar tab has grown to match.
- Recovery days are getting longer. The hangover from cocaine plus alcohol is noticeably worse than from either alone. Monday is a write-off. Sometimes Tuesday is too.
- Chest pain, palpitations, or nosebleeds. These are physical warning signs that the cardiovascular stress is causing real damage.
- Financial impact. A cocaine-and-alcohol habit is expensive. If you’re spending more than you can afford, that’s a dependency signal.
- Personality changes. Irritability, paranoia, mood swings, withdrawal from relationships — these often worsen with polydrug use.
If three or more of these apply, the combination has moved past recreational use. The earlier it’s addressed, the less physical and psychological damage accumulates.
Concerned about cocaine and alcohol use — yours or someone else’s? Talk to our team — we’ll give you a straight answer about what level of help is needed.

How Is Cocaine and Alcohol Addiction Treated Together?
Cocaine and alcohol addiction must be treated simultaneously within a single programme because the two substances are pharmacologically and psychologically intertwined. Treating cocaine use while ignoring alcohol — or vice versa — leaves half the addiction active and virtually guarantees relapse. Effective treatment combines medically supervised detox (primarily for alcohol withdrawal), structured therapy addressing both substances, and relapse prevention that accounts for the linked triggers.
At One Step, the programme works like this:
First 3–7 days: Stabilisation. Alcohol withdrawal is the medically dangerous part. Cocaine withdrawal is uncomfortable — fatigue, depression, intense cravings — but not life-threatening. If you’ve been drinking heavily, your first days focus on medical oversight during alcohol detox, with regular check-ins and medication management where needed. Cocaine cravings are managed through structure, physical activity, and clinical support.
Weeks 1–4: Core therapy. Once stable, you enter the full treatment programme. This includes CBT and DBT sessions that specifically address the cocaine-alcohol link — identifying triggers, breaking the association between the two substances, and building alternative responses. Group therapy connects you with others who understand polydrug use. Individual sessions dig into the personal patterns driving the behaviour.
The daily structure matters. The treatment schedule runs from 7am through evening programming. Morning meditation, group therapy sessions, individual counselling, fitness, and activities and excursions fill the day. There’s no unstructured downtime where cravings can take hold.
What it costs. One Step charges approximately ฿280,000/month (~$8,500 USD). That covers accommodation (private room with AC), all therapy, medical oversight during detox, meals, fitness, and weekend excursions. It doesn’t cover flights, personal spending, or optional extras. Full details are on the pricing page.
What happens after. The aftercare programme continues support after you leave. This is especially important for cocaine-alcohol combinations because the triggers are social — the same bars, the same friends, the same Friday night routines that led to use.
Honest limitations. We’re a mid-range residential facility, not a hospital. For severe alcohol withdrawal with a history of seizures or delirium tremens, we may detox you first at our partner hospital — which has intensive and intermediary intensive care units — before you transfer to One Step for the rehab programme. We’ll tell you that during the admissions assessment rather than admitting someone we can’t safely manage.

What Does Withdrawal From Cocaine and Alcohol Look Like?
Withdrawal from combined cocaine and alcohol use involves two overlapping but different processes. Alcohol withdrawal produces physical symptoms — tremors, sweating, elevated heart rate, potential seizures — that peak at 24–72 hours and require medical monitoring. Cocaine withdrawal is primarily psychological — profound fatigue, depression, vivid dreams, intense cravings — that can persist for weeks. Managing both simultaneously requires careful clinical attention.
| Factor | Alcohol withdrawal | Cocaine withdrawal |
|---|---|---|
| Onset | 6–12 hours after last drink | Hours to days after last use |
| Peak severity | 24–72 hours | 3–7 days |
| Physical symptoms | Tremors, sweating, nausea, seizures, elevated blood pressure | Fatigue, increased appetite, physical slowing |
| Psychological symptoms | Anxiety, confusion, hallucinations (in severe cases) | Depression, intense cravings, irritability, vivid nightmares |
| Medical danger | High — seizures and delirium tremens can be fatal | Low — uncomfortable but not life-threatening |
| Duration | Acute phase: 5–7 days | Acute phase: 1–2 weeks; cravings can persist for months |
The challenge with dual withdrawal is that as alcohol withdrawal subsides (days 5–7), cocaine cravings often intensify. The brain has adjusted to receiving both substances, and the absence of cocaine’s dopamine surge on top of the depleted state from alcohol withdrawal can create a particularly difficult window. This is when structured therapeutic support matters most — and when people in outpatient settings most commonly relapse.
At One Step, the first week balances medical attention for alcohol withdrawal with gentle re-engagement in daily structure. As the acute phase passes, therapy intensity increases progressively. You’re never discharged between detox and residential rehabilitation — it’s one continuous stay.

What Are the Long-Term Health Effects of Using Cocaine and Alcohol Together?
Long-term combined use of cocaine and alcohol causes cumulative damage to the heart, liver, and brain that exceeds the harm from either substance alone. Cocaethylene is more toxic to the liver than cocaine and contributes to liver inflammation and damage over time. The repeated cardiovascular stress increases the risk of heart disease, stroke, and heart failure — risks that build with every session of combined use (Jones, J Anal Toxicol, 2019).
Specific long-term risks include:
- Heart damage: Repeated cocaethylene exposure strains the heart muscle. Over time this can lead to cardiomyopathy (weakened heart muscle), arrhythmias, and increased risk of heart attack — even in people in their 20s and 30s.
- Liver damage: The liver is doing triple duty — processing alcohol, processing cocaine, and producing cocaethylene. Animal studies show that cocaethylene has a lower lethal dose than cocaine, meaning it is more toxic per unit (Jones, J Anal Toxicol, 2019).
- Brain changes: Both substances independently alter the brain’s dopamine system. Combined long-term use can produce lasting changes in motivation, pleasure, impulse control, and emotional regulation.
- Mental health deterioration: Anxiety, depression, paranoia, and cognitive impairment are all more pronounced with polydrug use. The “crash” after combined use is often severe enough to interfere with work and relationships for days.
- Nasal and respiratory damage: If cocaine is snorted, the combination of cocaine’s vasoconstrictive effects and alcohol’s inflammatory effects accelerates damage to nasal passages and can worsen breathing problems from smoking crack.
The good news: much of this damage is reversible with sustained abstinence, particularly in younger users. Cardiac function typically improves once the substances are removed. Liver markers normalise. Cognitive function gradually recovers. But the longer combined use continues, the more permanent the damage becomes.

If you or someone you love is struggling with substance dependence, explore how a drug addiction treatment programme can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions About Cocaine, Alcohol, and Cocaethylene
Common questions about the risks of mixing cocaine and alcohol and how treatment works.
Yes. Combining cocaine and alcohol produces cocaethylene, which significantly increases the risk of cardiac arrest and sudden death. Emergency room data shows a ninefold increase in cardiac arrest among patients with cocaethylene in their system compared to cocaine alone. The combination also increases the risk of stroke, seizures, and fatal heart rhythm disturbances.
Cocaethylene has an elimination half-life of approximately 2 hours, compared to about 1 hour for cocaine. This means it remains active and detectable in your blood for several hours longer than cocaine alone. After a session of combined use, cocaethylene can be detected in blood for 12 or more hours, and its breakdown products persist even longer in urine.
In several important ways, yes. Cocaethylene blocks cardiac sodium channels more potently than cocaine, has a lower lethal dose in animal studies, and stays active in the body for roughly twice as long. While its subjective effects may feel slightly less intense than cocaine, its impact on the heart is measurably worse. The real danger is that cocaethylene is produced alongside cocaine — so when both are present, total toxicity is higher than either alone.
Yes, and the combination is often harder to break than either addiction alone. The two substances become psychologically linked — alcohol triggers cocaine cravings and cocaine triggers the urge to drink. Cocaethylene also produces its own reinforcing dopamine surge, creating a third layer of neurochemical reward. Effective treatment must address both substances simultaneously.
Treatment at One Step is a residential programme that addresses both substances from the start. The first 3–7 days focus on medically supervised alcohol detox and cocaine withdrawal management. Once stable, you enter daily structured therapy including CBT, DBT, group sessions, individual counselling, and fitness. Most stays are 28–60 days. The programme costs approximately ฿280,000/month (~$8,500 USD) and includes accommodation, all therapy, medical oversight, meals, and activities.
Yes — cocaethylene forms whenever cocaine and alcohol are both present in the body, regardless of which one was consumed first. However, drinking alcohol before using cocaine tends to produce more cocaethylene because the ethanol is already being processed when the cocaine reaches the liver. The order and timing affect how much cocaethylene is produced, but any overlap creates it.
Much of the damage is reversible with sustained abstinence, especially in younger users. Cardiac function typically improves once both substances are removed. Liver function markers return to normal. Cognitive function and mental health gradually recover over weeks and months. However, the longer combined use continues, the greater the risk of permanent damage. Early treatment significantly improves long-term health outcomes.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








