
Key Takeaways
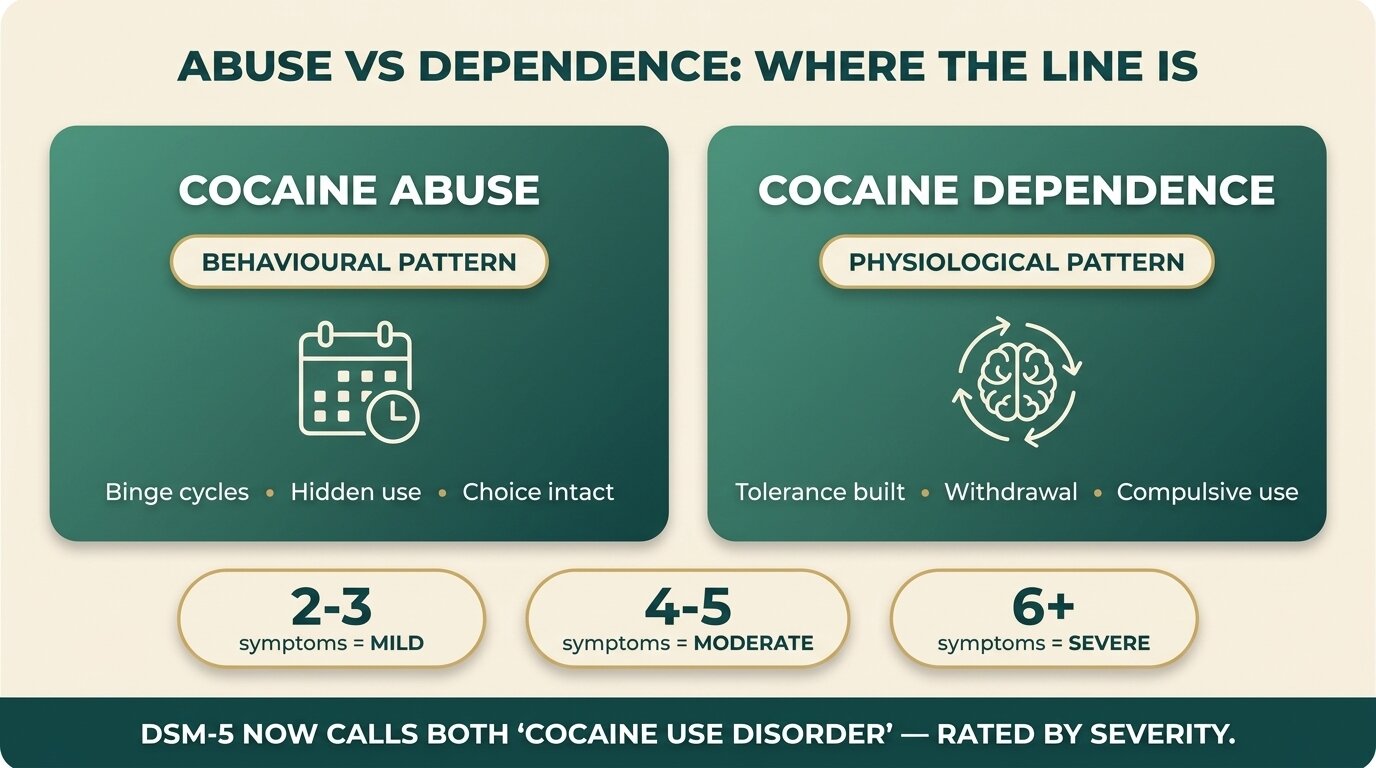
- The DSM-5 dropped the old “abuse vs dependence” split in 2013 and now uses one diagnosis — Cocaine Use Disorder (CUD) — rated mild, moderate, or severe based on how many of 11 symptoms a person ticks.
- The old categories still describe two real patterns: abuse = a behavioural problem (binges, hidden use, social and work fallout); dependence = a physiological problem (tolerance, withdrawal, compulsive use).
- The line is crossed when your body stops giving you the choice — when stopping causes a crash, sleep collapse, and depressive symptoms strong enough that using again feels like relief, not a decision.
- “Abuse” is not the sub-clinical tier. Mild CUD still wrecks careers, finances, and relationships. Both patterns need treatment — only the intensity of the intervention differs.
- Self-assessment markers (frequency, tolerance, withdrawal, control) help you understand where you are; only a clinician can diagnose. If you can’t predict how the next binge will end, you need help.
The clinical world stopped separating cocaine abuse and cocaine dependence in 2013, when the DSM-5 collapsed both into a single diagnosis — Cocaine Use Disorder — graded mild, moderate, or severe (SAMHSA, 2016). But the older DSM-IV split — abuse on one side, dependence on the other — is still useful if you’re trying to understand your own use or a family member’s. Abuse describes a behavioural pattern: cocaine causes problems but you can still choose. Dependence describes a physiological pattern: your brain has adapted, stopping makes you sick, and “choice” has narrowed to almost nothing. The line between them is the point where pattern becomes physiology.
Why Did the DSM Stop Splitting Cocaine Abuse and Dependence?
The DSM-5 merged the two categories because the data didn’t support a clean wall between them. A 2014 study of cocaine users found that DSM-IV “abuse” cases overlapped substantially with mild dependence on symptom count, time spent using, and impairment — meaning the labels described a continuum, not two separate diseases (Proctor, Psychology of Addictive Behaviors, 2014).
Under the old system, “abuse” was diagnosed when cocaine caused problems — failing at work, legal trouble, relationship damage, dangerous use — without requiring withdrawal or tolerance. “Dependence” added the physical layer: needing more, getting sick when you stopped, losing the ability to control how much you used. A clinician had to pick one. The two categories felt clean on paper but were messy in practice — most people who met abuse criteria eventually met dependence criteria, and many people sat in a grey zone the DSM-IV couldn’t name.
The DSM-5 fixed this by listing 11 symptoms and counting them. Two or three symptoms is mild CUD. Four or five is moderate. Six or more is severe. The 11 symptoms cover four areas: impaired control (using more than intended, can’t cut down), social impairment (problems at work, with family, in relationships), risky use (using in dangerous situations, knowing it’s hurting you), and pharmacology (tolerance, withdrawal). The new system is more honest about how addiction actually unfolds — it’s a slope, not a step.
What Did “Cocaine Abuse” Actually Describe?
Cocaine abuse, under DSM-IV, described problematic use without physical dependence: weekend binges that wreck Monday performance, hidden use that breaks trust, drug-driving, lost jobs, blown budgets. The body hadn’t yet adapted — you could stop for weeks without withdrawal — but cocaine was reliably causing harm and you kept using anyway.
In real life, abuse looks like this:
- The weekend pattern. Heavy use Friday through Sunday, recovery Monday and Tuesday, restraint Wednesday and Thursday, then back at it. No tolerance build-up, no daily withdrawal — but the weekly cost (money, sleep, mood) compounds.
- The binge-and-stop cycle. Three-day runs every few weeks, then nothing. Genuinely no use between binges. But each binge is longer or heavier than the last, and the recovery period stretches.
- The functional user. Performs at work, looks fine to outsiders, uses cocaine to maintain energy, social confidence, or focus. The damage is privatised — credit-card debt, relationship cracks, secrets — but visible function holds.
- The contextual user. Only uses in specific situations (clubs, parties, certain friend groups) but cannot attend those situations without using. The trigger isn’t the drug — it’s the context — but the user has lost the ability to opt out.
In every case, the person could still choose not to use on a given Tuesday morning. That choice is what separates abuse from dependence. But “could choose” doesn’t mean “isn’t sick” — it means the disease is at an earlier stage, where intervention is easier and the cost of waiting is lower.
What Did “Cocaine Dependence” Look Like in the Body?
Cocaine dependence described the point where the brain had adapted to chronic exposure — tolerance built, dopamine production blunted, and stopping triggered a recognisable withdrawal syndrome of crash, depression, sleep disturbance, and intense craving. At that stage, “using again” stopped being a free choice and started being a way to escape a physiological state (NIDA, 2024).
Three physical signs separate dependence from abuse:
| Marker | What you notice | What’s happening underneath |
|---|---|---|
| Tolerance | Needing larger amounts or more frequent use to get the same effect. Old doses feel underwhelming or pointless. | The brain has down-regulated dopamine production and receptors. The same dose now produces a smaller spike against a flatter baseline. |
| Withdrawal | After 12–72 hours without cocaine: exhaustion, oversleeping, intense hunger, depressed mood, anxiety, and powerful cravings. Sometimes vivid bad dreams. | Dopamine and serotonin systems crash below baseline. Stress circuits become hypersensitive — everything feels worse than it should. |
| Compulsive use | Using when you don’t want to. Using during work hours, alone, in situations that violate your own rules. “I’ll stop after this gram” repeating for weeks. | The orbitofrontal cortex — the part of the brain that weighs consequences — has been impaired by chronic use, narrowing the gap between urge and action. |
The withdrawal isn’t dangerous in the way alcohol or benzodiazepine withdrawal can be — no seizures, no delirium tremens — but it is brutal enough that most people relapse to escape it. That’s the trap. The person isn’t using to get high any more; they’re using to stop feeling subhuman.

Where Is the Line Between Abuse and Dependence?
The line is crossed when your body stops giving you the choice. Specifically: when stopping triggers a crash strong enough that using again feels like relief rather than a decision, when tolerance forces dose escalation, and when use continues during periods you’d previously kept clean. Abuse is “I keep doing this even though it’s hurting me.” Dependence is “I can’t stop, and stopping makes me sick.”
Useful self-assessment questions:
- Tolerance check. Are you using more cocaine per session or more often than you did six months ago to get the same effect? Yes = a dependence marker.
- Withdrawal check. When you stop for 48–72 hours, do you crash — heavy sleep, depressed mood, intense craving, low energy? Yes = a dependence marker.
- Control check. Do you finish a bag/binge faster or more often than you intended to? Have you broken your own rules (no weekdays, no using alone, no using after a certain time) in the last 30 days? Yes = a dependence marker.
- Time check. How many hours per week are spent using, recovering, getting, or thinking about cocaine? More than ten hours suggests the pattern has moved beyond casual.
- Stop test. Could you stop for 30 days right now if you had to? Not “would you want to” — could you? If the answer is no, or if the answer is “yes but I’d be miserable,” you’re in dependence territory.
None of this is a diagnostic tool. A clinician using the full DSM-5 criteria is the only person who can give you a severity rating. But these questions are accurate enough to tell you whether you need help, and how soon.
People often arrive convinced that they have a discipline problem — that they just need to use less or use better. What we usually find is that the discipline ran out long ago, and what they’re really fighting is a brain that has adapted to expect cocaine. Once tolerance and withdrawal are in the picture, willpower is the wrong tool. The right tool is structured treatment that gives the brain time and the right inputs to recalibrate.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Not sure which pattern fits you? Talk to our team — we’ll walk you through where you are and what level of help would actually move the needle.

Why Does the Old Distinction Still Matter If the DSM Dropped It?
The old categories still matter because they describe two genuinely different problems that need different treatment intensities. Mild CUD (formerly “abuse”) often responds to outpatient counselling, structured peer support, and behavioural change. Moderate to severe CUD (formerly “dependence”) usually requires residential treatment to break the daily-use loop and stabilise the brain before any therapy can land.
The risk with collapsing everything into one diagnosis is that “Cocaine Use Disorder” can sound either too clinical for someone with a weekend problem (“I’m not an addict, I just party”) or too soft for someone in physical dependence (“It’s just a disorder, I’ll manage it”). The DSM-5 fix is the severity rating — mild, moderate, severe — but most people don’t know their rating, and the term “use disorder” doesn’t carry the weight that “dependence” did.
Practical implications of where you sit on the spectrum:
| DSM-5 Severity | Closest DSM-IV equivalent | Typical treatment match |
|---|---|---|
| Mild (2–3 symptoms) | Cocaine abuse | Outpatient counselling, CBT, peer support (SMART Recovery, CA). Behavioural change before physiology hardens. |
| Moderate (4–5 symptoms) | Border zone — late abuse / early dependence | Intensive outpatient or short residential. Address tolerance and emerging withdrawal before they entrench. |
| Severe (6+ symptoms) | Cocaine dependence | Residential treatment (28–90 days). Time away from triggers, supervised early abstinence, daily therapy. |
One thing to be clear about: mild CUD is not the safe tier. The literature is consistent that severity at entry predicts outcomes — people with more severe addiction relapse at higher rates and respond more slowly to treatment — but mild CUD still ends careers, destroys relationships, and progresses to severe if untreated (Palazón-Llecha et al., Systematic Reviews, 2024). The reason to act on mild CUD isn’t because it’s worse than it looks — it’s because it’s the easiest stage to treat.
When Does Each Pattern Need Treatment?
Mild CUD (cocaine abuse) needs help when the pattern stops being correctable on your own — when you’ve tried to cut down and couldn’t sustain it, when use is bleeding into areas you’d ringfenced, or when the consequences (financial, legal, relational) are stacking up. Severe CUD (cocaine dependence) needs help immediately — the longer dependence runs, the more entrenched the neuroadaptations become and the harder the climb out gets.
Specific triggers to act on, whichever pattern fits:
- Failed self-correction. You set a rule (no weekdays, no using alone, weekend-only), kept it for a while, and it collapsed. One failure is data. Two is a pattern. Three means the problem is bigger than your rules.
- Hidden use. Lying to a partner, a parent, or yourself about how much or how often you use. Secrecy is one of the earliest reliable markers that use has crossed into problem territory.
- Crash recovery. If your “normal” Monday or Tuesday is a recovery day — flat mood, no energy, can’t engage at work — that’s a withdrawal pattern, even if you haven’t named it that.
- Money flow. Cocaine spending exceeding what you’d consciously approve, debt accumulating, or money going missing in ways you’d be embarrassed to explain. This is often the first signal that hits a partner before they realise what they’re seeing.
- Co-use escalation. Drinking more alongside cocaine — especially binge drinking — multiplies cardiovascular risk and creates cocaethylene, a more toxic third compound the liver makes when both are on board.
- Method change. Moving from snorting powder to crack or freebase is almost always a sign that tolerance has built and the user is chasing a stronger or faster hit. Method change usually precedes severity escalation.

How Does One Step Approach Cocaine Use Disorder?
At One Step’s cocaine rehab programme, we treat CUD as a spectrum rather than two categories, but we calibrate the intensity of treatment to where you actually are. Mild cases get a different programme density than severe cases — same modalities, different dose.
Practical details:
- Detox happens on-site. Cocaine withdrawal is unpleasant but not medically dangerous — no seizures, no delirium tremens. We handle the first week with medical oversight, sleep support, nutrition, and structured downtime. No partner hospital transfer required.
- Length of stay. Most cocaine clients stay 28–60 days. Severe CUD with long binge histories or polysubstance use usually needs 60–90 days. Anything under 28 rarely holds.
- Therapy. The programme runs on CBT and DBT with daily group sessions and one-to-one counselling. Cocaine recovery in particular benefits from skills work on craving management and trigger mapping. The role of therapy in cocaine recovery covers this in depth.
- Cost. ฿280,000/month (~$8,500 USD). Medication, flights, visa fees, and personal items are billed separately. See the pricing page for the full inclusion list.
- Daily structure. Wake at 7am, group therapy mid-morning, individual sessions, gym or outdoor activities afternoon, evening reflection. The treatment schedule page has the full weekly grid.
- Aftercare. Cocaine has high relapse rates in the first 12 months — relapse risk peaks around the 90-day mark when the brain hasn’t fully recalibrated but the structured support of treatment is gone. Aftercare includes weekly check-ins and an alumni network specifically to bridge that window.
The 50% one-year relapse rate for stimulants is the figure clinicians work with (Palazón-Llecha et al., Systematic Reviews, 2024). The strongest predictors of staying in the 50% who don’t relapse are length of stay in initial treatment and engagement with aftercare. Neither is about willpower; both are about structure.
If you or someone you love is struggling with substance dependence, explore how a drug addiction treatment in Thailand can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions about cocaine abuse, cocaine dependence, and the modern Cocaine Use Disorder diagnosis.
Less physiologically entrenched, not less serious. Abuse (mild CUD) describes a behavioural pattern where the brain hasn’t yet built tolerance or withdrawal, but the consequences — money, work, relationships — can be just as damaging. The reason to take it seriously is that mild CUD is the easiest stage to treat and the highest-yield stage to intervene.
Yes. Many people in cocaine dependence binge for two to four days, crash hard, recover for a week, then binge again. Daily use isn’t required for tolerance and withdrawal to develop — repeated heavy binge cycles can produce the same neuroadaptations. The pattern of use matters less than the brain’s response to it.
The DSM-5 criteria cover four areas: impaired control (using more than intended, failed attempts to cut down, time spent using, craving), social impairment (failing role obligations, relationship damage, giving up activities), risky use (using in dangerous situations, continuing despite harm), and pharmacology (tolerance, withdrawal). Two or three symptoms is mild, four to five moderate, six or more severe.
The acute crash phase lasts 1–3 days — heavy sleep, hunger, exhaustion, low mood. The longer recovery phase, where mood, energy, and sleep are still flatter than baseline, runs roughly 2–10 weeks depending on use history. Cravings can recur for months. The pattern isn’t physically dangerous like alcohol withdrawal, but it’s the main reason people relapse on their own.
Not always. Mild CUD often responds to structured outpatient counselling, CBT, and peer support if you have a stable environment and your use hasn’t broken into work hours. Residential becomes the right answer when outpatient has failed, when the home environment is itself a trigger, or when the pattern is escalating faster than you can address it from inside your life.
No. No medication is currently approved as a substitute or maintenance treatment for cocaine use disorder. Behavioural therapies — particularly contingency management and CBT — are the first-line interventions. Adjunctive medications are sometimes used to manage co-occurring depression, sleep disruption, or anxiety, but they treat the side effects, not the dependence itself.
Because most people aren’t reading the DSM. The words “abuse” and “dependence” still carry meaning that “mild use disorder” doesn’t — they communicate something about whether the body has adapted or not. Clinicians use the DSM-5 severity system; the older terms remain useful as a translation layer for people trying to understand themselves or a family member.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








