
Key Takeaways
- The most distinctive harm of chronic ketamine abuse is bladder damage — ketamine-induced ulcerative cystitis can progress to a small, scarred, contracted bladder that surgery cannot reverse.
- In severe cases, the endpoint is bladder removal (cystectomy) or urinary diversion. Ureter and kidney damage can follow, with some patients requiring dialysis.
- Heavy users show measurable declines in episodic memory, spatial working memory and pattern recognition — and dose-response increases in dissociative and depressive symptoms over a year of use.
- Fatal overdose from ketamine alone is rare. In US overdose data, ketamine was the only substance in 0.01% of deaths; 82% of ketamine-detected deaths involved other drugs.
- The real overdose risk comes from combinations — alcohol, GHB, opioids and benzodiazepines stack respiratory depression on top of ketamine’s dissociation.
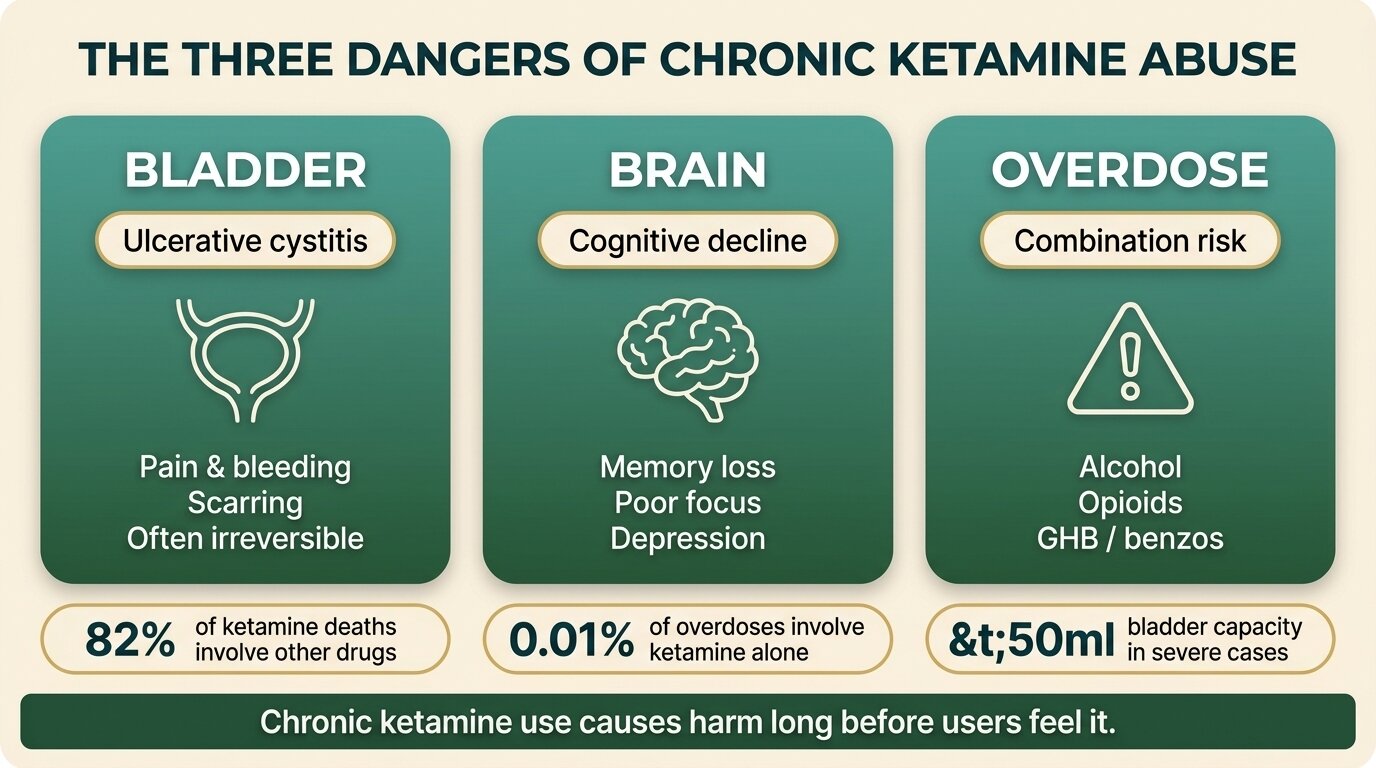
The dangers of ketamine abuse are not what most users expect. Ketamine rarely kills on its own — but heavy, sustained use causes a specific, progressive bladder disease that can leave young people incontinent, in chronic pelvic pain, or facing bladder removal in their twenties. It also degrades memory and executive function, and turns dangerous when stacked with alcohol, GHB, benzodiazepines or opioids (NIDA, 2024).
The picture has shifted in the last decade. A generation of recreational users started with weekend bumps and ended up in urology clinics — first with painful, bloody urination, then with bladders so scarred they hold less than 50ml. The damage is the most under-discussed part of ketamine, partly because it doesn’t fit the older “ketamine is the safe one” narrative.
This post covers the three pillars of chronic ketamine harm — bladder, brain and overdose risk — based on the urology, psychiatry and toxicology literature, and on what we see in clients presenting for treatment at One Step Rehab in Chiang Mai.
What Is Ketamine Bladder and How Bad Does It Get?
Ketamine bladder, known clinically as ketamine-induced ulcerative cystitis or ketamine-induced uropathy, is severe inflammation and scarring of the bladder wall caused by ketamine and its metabolites attacking the protective lining. It progresses through frequent painful urination, blood in the urine and intense bladder spasms (“K-cramps”), to a small, fibrotic bladder that cannot stretch or refill normally (Castellani et al., Neurourol Urodyn, 2020).
The first case series was published in 2007: nine young, daily ketamine users presenting with severe dysuria, urgency, frequency and visible blood in the urine. All had sterile urine cultures and thickened bladder walls (Shahani et al., Urology, 2007). The following year, Chu and colleagues in Hong Kong described 59 abusers and named the contracted-bladder syndrome — with a subset showing kidney damage so severe it left them dialysis-dependent (Chu et al., BJU Int, 2008).
The stages, roughly, look like this:
| Stage | What the user notices | What is happening | Reversibility |
|---|---|---|---|
| Early irritation | Urgent need to urinate, mild burning, going more often | Inflammation of the bladder lining | Usually reverses with abstinence |
| Ulcerative cystitis | Severe pain on urinating, blood in urine, getting up many times a night, incontinence | Ulceration of the bladder wall, loss of protective coating | Often improves with abstinence and treatment if caught here |
| Contracted bladder | Tiny bladder capacity (sometimes <50ml), constant pelvic pain, K-cramps | Fibrosis (scarring) replaces normal bladder tissue | Largely irreversible — surgery may be needed |
| Upper-tract involvement | Flank pain, signs of kidney damage | Backflow into ureters; hydronephrosis; renal scarring | Can progress to dialysis in severe cases |
Once the bladder is fibrotic and contracted, stopping ketamine no longer restores it. The endpoint for the worst cases is surgical augmentation cystoplasty (enlarging the bladder using a piece of bowel), cystectomy (removing the bladder), or urinary diversion to a stoma bag (Jalil et al., BMJ Case Rep, 2012). The patients are often in their early twenties.
This is the single most important fact about chronic ketamine use, and the one most users discover too late: the damage is real, it accelerates fast, and after a certain point, no amount of abstinence will bring the bladder back.

How Does Heavy Ketamine Use Affect the Brain?
Heavy ketamine use is linked to measurable cognitive decline, especially in memory and executive function. A one-year longitudinal study of frequent users found that increasing ketamine use over the year tracked with worsening spatial working memory and pattern recognition memory — and with dose-related increases in dissociative symptoms, delusional thinking and depression (Morgan et al., Addiction, 2010).
In plain terms, what we see clinically and what the research shows:
- Episodic memory deficits. Heavy users have trouble laying down and retrieving day-to-day memories — what happened yesterday, where they left things, what was said in a conversation last week.
- Executive function decline. Planning, holding multiple things in mind at once, switching between tasks, and inhibiting impulses all get harder. This is the same set of skills people need to hold down a job, manage money, and stay in treatment.
- Persistent dissociation. Frequent users describe feeling “blank” or “behind glass” even when they haven’t used in days. This is the same dissociative state ketamine produces acutely — just lingering between use.
- Depression and delusional symptoms. Both rise with heavier use and don’t fully resolve on the timescale of a one-year follow-up.
The cognitive picture is not as terminal as the bladder picture — some impairments improve substantially after extended abstinence. But the people in the worst shape clinically are usually using daily, often hourly, and the damage matches the dose.

Can You Overdose on Ketamine?
Yes, but fatal overdose from ketamine alone is rare. In a CDC analysis of 228,668 US overdose deaths between July 2019 and June 2023, ketamine was detected in 912 deaths (0.4%) — and was the only substance in just 24 of those (0.01%). Roughly 82% of ketamine-involved deaths included other drugs, most commonly illicitly manufactured fentanyl, methamphetamine, cocaine, benzodiazepines, opioids or alcohol (Vivolo-Kantor et al., MMWR, 2024).
That framing matters. The danger isn’t a single bump — it’s the combination. Ketamine on its own produces dissociation, slowed breathing and a depressed gag reflex. Stack it with another depressant and the risk profile changes:
| Combination | What goes wrong |
|---|---|
| Ketamine + alcohol | Both depress breathing and gag reflex. Vomiting in a dissociated state has caused fatal aspiration. About 71% of US ketamine-related ER visits in 2011 involved alcohol. |
| Ketamine + GHB/GBL | Both cross-potentiate sedation and respiratory depression. Animal data show ketamine prevents the compensatory breathing increase GHB normally allows — co-use is more lethal than either alone. |
| Ketamine + opioids (heroin, oxycodone, fentanyl) | Opioids cause the respiratory arrest; ketamine masks the cues that something is wrong and impairs the ability to call for help. |
| Ketamine + benzodiazepines | Two CNS depressants stacking. Reduces consciousness to the point where airway protection fails. |
| Ketamine + stimulants (MDMA, cocaine, meth) | Not classically lethal via respiratory depression, but cardiovascular strain, hyperthermia and dehydration. Users miss warning signs because of dissociation. |
The other under-recognised risk is the dissociated state itself. Someone in a deep k-hole cannot reliably protect their airway, cannot call for help, and cannot move out of danger. People drown in baths, suffocate face-down in pillows, choke on vomit. The substance didn’t kill them in a pharmacological sense — being too dissociated to react did.
The thing that makes ketamine so deceptive is that the worst harm is silent. The bladder is being destroyed for months before most users notice anything beyond “going to the loo a bit more.” By the time the pain forces them to stop, the scarring can already be permanent. We’re seeing people in their mid-twenties with the urinary function of an eighty-year-old.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Already noticing urinary symptoms or daily use you can’t stop? Talk to our team — we’ll give you a straight answer about whether residential treatment makes sense for your situation.
Why Are These Dangers So Underestimated?
The dangers of ketamine abuse are underestimated because ketamine arrived with a reputation it no longer deserves. For most of the 1990s and 2000s it was framed as one of the “safer” party drugs — short-acting, non-cardiotoxic, with low overdose risk on its own. That framing aged badly. The urology literature only started catching up in 2007, and the harm picture has since shifted toward chronic, irreversible damage that none of the older harm-reduction guides described.
The UK reflects this clearly. The Advisory Council on the Misuse of Drugs originally moved ketamine to Class B in 2014 specifically because of the rising evidence of bladder damage from frequent use. In January 2026 the ACMD reviewed the case for upgrading it again to Class A and decided against it — keeping the classification but emphasising that the long-term harms, especially from high-dose daily use, are growing (ACMD / GOV.UK, 2026).
Two other reasons the harms get missed:
- The bladder damage hides as a urinary tract infection. Early symptoms — frequency, urgency, painful urination — match a UTI almost exactly. Users often cycle through repeated negative urine cultures and rounds of antibiotics before anyone asks about ketamine.
- Medical ketamine looks like a safety endorsement. Esketamine is now used for treatment-resistant depression. Ketamine is a frontline anaesthetic worldwide. Recreational users read this as evidence the drug is benign, missing the gap between supervised single doses and daily recreational use measured in grams.
For a closer look at why people start with ketamine in the first place, our guide on how ketamine makes you feel and the K-hole covers the acute effects in detail.
When Should Someone Be Worried About Their Ketamine Use?
The clearest warning signs are urinary symptoms, escalating frequency of use, and use that has shifted from social weekends to solitary daily dosing. Any urinary changes — pain, urgency, blood, going more often than peers — in a regular ketamine user should be treated as ketamine bladder until proven otherwise, not as a routine UTI. Early urological assessment is the single thing that most changes the long-term outcome.
Other patterns we see in clients arriving for treatment:
- Going from key bumps on a night out to half a gram or more a day, often via nasal use throughout the day
- Carrying ketamine “for the cramps” — using more ketamine to mask the bladder pain that ketamine is causing
- Memory blanks, missed conversations, having to be reminded of recent events
- Withdrawing from people who don’t use, because dissociation feels easier than engagement
- Combining with alcohol, MDMA, GHB or benzodiazepines because tolerance has flattened the ketamine effect
- Trying to stop and failing — not for classic withdrawal reasons, but because the dissociation has become emotionally load-bearing
For families and partners who suspect use, our companion guide on warning signs of ketamine addiction in teens covers what to look for and how to raise it.
How Does One Step Treat Chronic Ketamine Use?
One Step Rehab treats ketamine addiction in our standard 28-to-60-day residential programme in Chiang Mai. Ketamine doesn’t produce a severe physical withdrawal in the way heavy alcohol or benzodiazepine dependence does, so detox happens on-site rather than at a hospital. The harder work is the psychological piece — managing cravings, treating the underlying anxiety, depression or trauma that ketamine was numbing, and rebuilding executive function over weeks of structured days.
What that looks like in practice at One Step:
- Intake and medical screening. Our visiting psychiatrist reviews medical and psychiatric history, and we screen urinary symptoms because so many heavy ketamine users have undiagnosed bladder damage. If symptoms suggest ketamine cystitis, we arrange a urology assessment locally — early urological care often determines whether damage is reversible.
- On-site stabilisation. Ketamine cravings typically peak in the first two to three weeks. Phones are restricted in the early phase. Clients aren’t left alone to white-knuckle it — the day is structured from wake-up to lights-out.
- Therapy core. Daily group therapy and individual sessions using CBT and DBT approaches, focused on craving management, emotion regulation, and the dissociation-versus-engagement choice ketamine users have to relearn.
- Physical recovery. Daily activity (gym, hikes, swimming) and a high-protein, nutrient-dense diet — both help cognitive recovery in ways the literature on chronic users supports.
- Aftercare planning. Before discharge we build out a relapse-prevention plan and connect clients with ongoing aftercare support, because the first 90 days back home are where the relapse risk peaks.
The programme fee is around ฿280,000/month (~$8,500 USD). That covers accommodation, three meals a day, all on-site therapy, group sessions, activities and excursions. Medication prescribed by the doctor is billed separately, as are flights, visas, hospital visits and personal items — see our pricing page for the full inclusion and exclusion list, and our ketamine rehab page for more on the treatment pathway.
If you or someone you love is struggling with substance dependence, explore how a comprehensive drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions about the dangers of chronic ketamine abuse, bladder damage, cognitive harm and overdose risk.
Early-stage inflammation and ulcerative cystitis often improve with full abstinence and urological treatment. Once the bladder wall scars and becomes fibrotic and contracted, the damage is largely irreversible — at that point the management options are pain control, bladder augmentation surgery, or, in the worst cases, bladder removal and urinary diversion.
There is no safe daily dose established in the literature, but the case series describe damage in daily users consuming around a gram or more per day for months. Frequency and duration matter more than any single dose. Some users develop symptoms within a year of regular use; sensitivity varies considerably between individuals.
A K-cramp is an intense, doubled-over abdominal or pelvic pain that hits frequent ketamine users. It comes from the bladder, ureters and surrounding tissue under inflammation and spasm. Many users initially mistake it for an unrelated stomach issue — it is one of the most reliable signs that the urinary system is being damaged.
No. Alcohol and ketamine both depress breathing and the gag reflex, and both impair coordination. The combination accounts for a large share of ketamine-related emergency department visits, and aspiration from vomiting while dissociated has caused fatalities. Mixing ketamine with alcohol, GHB, opioids or benzodiazepines is where most ketamine deaths actually come from.
Heavy chronic users show clear deficits in episodic memory, spatial working memory and pattern recognition while using, and the deficits track with dose. Some impairment improves substantially after extended abstinence, but the picture for the heaviest users is less encouraging — full recovery is not guaranteed. Earlier and longer abstinence gives the brain the best chance.
Ketamine does not produce the dramatic physical withdrawal seen with alcohol or benzodiazepines, but it builds tolerance fast and produces strong psychological dependence. Heavy users describe craving the dissociation itself, not a physical symptom. Stopping is hard for behavioural and emotional reasons rather than detox reasons — which is exactly why structured residential treatment helps.
A urologist. Anyone using ketamine regularly who develops urinary symptoms — pain, urgency, blood in urine, going more often — should ask their GP for a urology referral and tell the urologist about the ketamine use. Treatment is far more effective in the earlier inflammatory stages than once the bladder has scarred.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








