
Key Takeaways
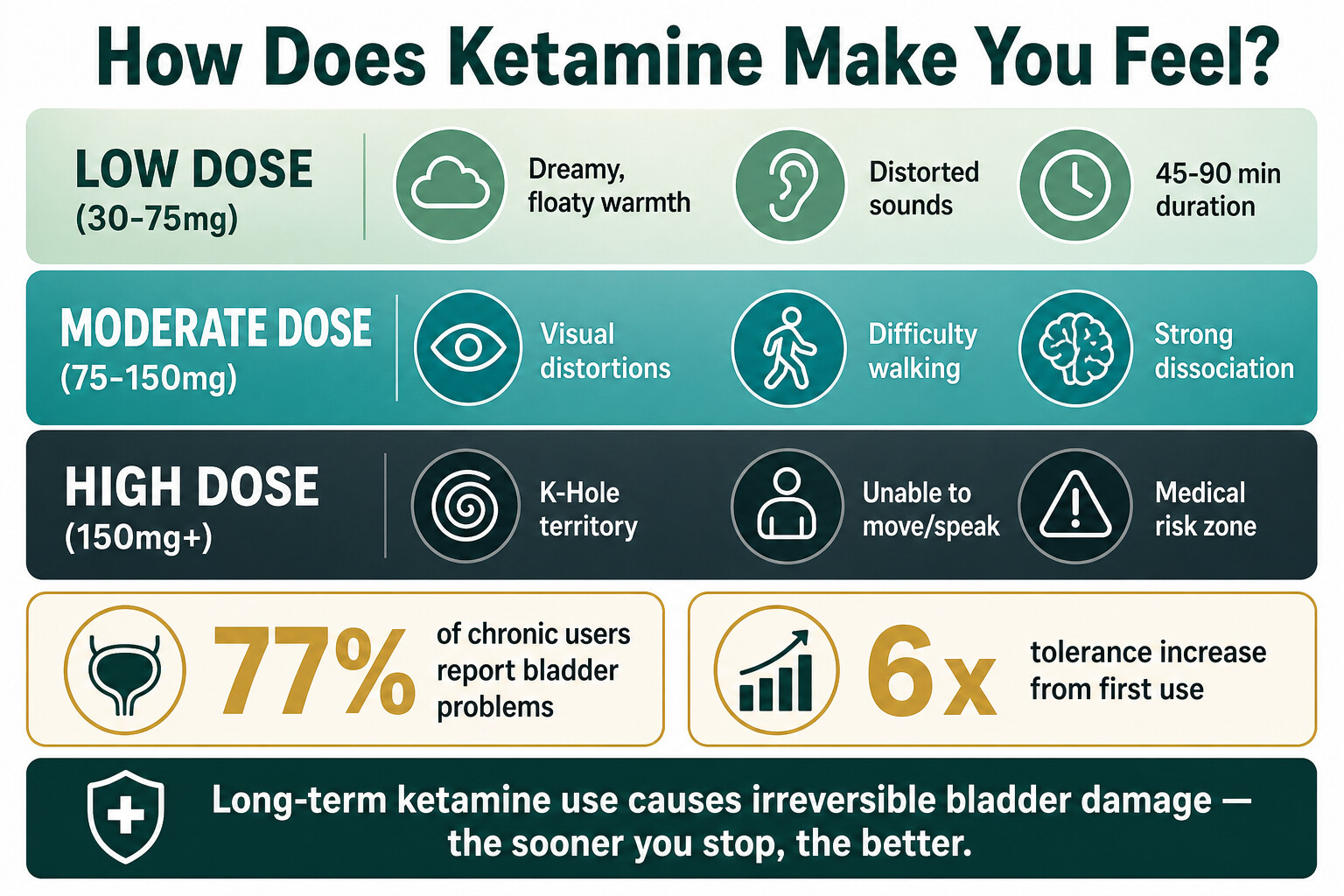
- At low doses, ketamine creates a floaty, dreamy feeling — distorted sounds, mild euphoria, and a sense of detachment from your body that lasts 45–90 minutes when snorted.
- Higher doses produce intense dissociation, visual hallucinations, and the “K-hole” — a state of near-total disconnection from reality that can feel like a near-death experience.
- Short-term physical risks include nausea, raised blood pressure, slowed breathing, and loss of coordination. Mixing with alcohol or downers is where most emergencies happen.
- Long-term, regular use damages the bladder (77% of chronic users report urinary problems), impairs memory, and builds tolerance fast — users commonly need six times their starting dose within months.
- Ketamine dependence is real but under-researched. Treatment focuses on structured therapy, not medication, because there’s no approved pharmacological treatment for ketamine use disorder.
Ketamine makes you feel detached — from your body, from your surroundings, sometimes from reality entirely. At lower doses, that means a dreamy, floaty warmth with distorted vision and sound. At higher doses, it means complete disconnection — unable to move, unable to speak, pulled into what users call the K-hole. It’s a dissociative anaesthetic, originally developed for surgery in the 1960s, and the effects reflect that: it doesn’t just alter your mood, it separates you from your senses (NIDA, 2024).
This post covers exactly what ketamine does to you at different doses, what the K-hole actually is, the physical risks most people underestimate, and what long-term use does to your bladder and brain. If you or someone close to you is using ketamine regularly, this is what you need to know.
What Does Ketamine Actually Feel Like?
At low recreational doses (typically 30–75 mg snorted), ketamine produces a warm, floaty sensation with mild euphoria, slurred speech, and distorted perception of sounds and colours. Users often describe feeling “drunk but different” — your body feels heavy while your mind feels light, and time seems to slow down or lose meaning. Effects begin within 5–15 minutes when snorted and last roughly 45–90 minutes (NIDA, 2024).
Unlike alcohol or opioids, ketamine doesn’t produce a straightforward “high.” It’s a dissociative — it works by blocking NMDA receptors in the brain, which disrupts the normal communication between your conscious mind and your senses. That’s why the experience often feels surreal rather than simply pleasurable. People report feeling like they’re watching themselves from outside their body, or that the room has become dreamlike and unfamiliar.
The specific experience varies significantly depending on the dose, the route of administration (snorted, injected, or swallowed), whether other substances are involved, and the person’s tolerance level. Someone using ketamine for the first time will feel markedly different effects than someone who has been using it weekly for months.
| Dose Range | What You Feel | Duration |
|---|---|---|
| Low (30–75 mg) | Mild euphoria, floaty feeling, slurred speech, distorted sounds | 45–90 min |
| Moderate (75–150 mg) | Strong dissociation, visual distortions, difficulty walking, confusion | 60–120 min |
| High (150 mg+) | K-hole territory — total disconnection, inability to move or speak, hallucinations | 1–3 hours |
| Injected (any route) | Faster onset, stronger effects at lower doses, harder to control | 15–60 min |
What Happens at Higher Doses of Ketamine?
At moderate to high doses, ketamine shifts from a dreamy buzz to full dissociation — your sense of self separates from your body, visual hallucinations become vivid, and you may lose the ability to walk, speak, or understand where you are. This isn’t like being “very drunk.” It’s a qualitatively different experience: users describe feeling like they’re dissolving into their surroundings, merging with objects, or entering entirely different realities (Muetzelfeldt et al., Drug Alcohol Depend, 2008).
At these doses, your body essentially becomes incapacitated while your mind enters a hallucinatory state. You can’t protect yourself — you can’t walk to safety, can’t call for help, and may not recognise danger. This is where injuries happen: falls, aspiration (inhaling vomit), and vulnerability to assault. The anaesthetic properties that make ketamine medically useful are the same ones that make high-dose recreational use dangerous — your pain response is suppressed, so you might not notice injuries until the drug wears off.
The transition from “pleasant buzz” to “unable to move” happens faster than most people expect, especially when redosing. Tolerance builds quickly with ketamine, and the dose that gave you a gentle float last week might not feel like enough this week — so you take more, and overshoot into territory you didn’t intend.

What Is a K-Hole?
A K-hole is a state of extreme dissociation caused by a high dose of ketamine, where you become almost completely disconnected from your body and environment. People who have experienced it describe being unable to move or speak, losing all sense of physical reality, and entering vivid hallucinatory spaces — tunnels, voids, fractal landscapes, or complete blankness. About two-thirds of regular ketamine users report that out-of-body experiences and visual hallucinations are among the drug’s most appealing effects, but the K-hole takes these far beyond what most users are seeking (Muetzelfeldt et al., Drug Alcohol Depend, 2008).
The term comes from recreational users and doesn’t have a formal medical definition, but it roughly corresponds to a near-anaesthetic dose — enough ketamine to approach the threshold of surgical anaesthesia without quite reaching full unconsciousness. You’re not asleep, but you’re not functionally awake either. Some people compare it to a near-death experience; others describe it as terrifying.
The K-hole typically lasts 30–60 minutes at its peak, with residual grogginess and confusion lasting several hours afterward. During the experience, users are physically helpless — unable to respond to their surroundings, unable to protect their airway if they vomit, and unable to communicate distress. The medical risk isn’t the dissociation itself (ketamine rarely causes fatal overdose when used alone), but the vulnerability it creates. Respiratory depression, aspiration, and injuries from the loss of motor control are the real dangers.
“What clients describe about the K-hole experience — the loss of control, the complete separation from reality — that’s essentially what ketamine was designed to do. It’s an anaesthetic. At high recreational doses, you’re self-administering a partial anaesthetic without medical supervision, airway monitoring, or anyone watching your vital signs. The margin between a dissociative high and a medical emergency is narrower than people realise.”
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
What Are the Physical Side Effects of Ketamine?
Short-term physical side effects of ketamine include nausea, vomiting, raised blood pressure, rapid heart rate, dizziness, blurred vision, and loss of coordination. Even at recreational doses, ketamine raises blood pressure and heart rate measurably — a concern for anyone with existing cardiovascular issues. Respiratory depression (dangerously slow, shallow breathing) is the most serious acute risk, especially when ketamine is combined with alcohol, opioids, or GHB (NIDA, 2024).
A NIDA-funded study found that problems related to ketamine use reported to US poison control centres increased 81% from 2019 to 2021. The most dangerous situations involved mixing ketamine with other depressants — opioids and GHB in particular led to the most life-threatening outcomes (NIDA, 2024). This is because ketamine already slows breathing, and combining it with other drugs that do the same thing can push breathing below the threshold your body needs to survive. Alcohol creates particular dangers when combined with stimulants — when mixed with cocaine, for example, the liver produces a toxic third compound called cocaethylene.
Other immediate effects people often don’t anticipate:
- Loss of pain response: Ketamine is an anaesthetic. You may not notice burns, cuts, or fractures until it wears off.
- Nausea and vomiting: Common, and dangerous if you’re too dissociated to turn your head.
- “K-cramps”: Severe abdominal pain that regular users know well — sharp, cramping pain in the stomach and abdomen.
- Inability to speak or call for help: At moderate-to-high doses, you lose the ability to communicate coherently.
Worried about your own or someone else’s ketamine use? Talk to our team — we’ll give you a straight answer about what kind of help makes sense.

What Does Long-Term Ketamine Use Do to Your Body?
Long-term regular ketamine use causes two major categories of damage: urinary tract destruction and cognitive impairment. The bladder damage is the more visible problem — a meta-analysis of 45 studies covering nearly 5,000 patients found that 77% of chronic ketamine users experience urinary frequency, 70% experience urgency, and 60% report severe pain above the pubic bone. Functional bladder capacity drops to an average of just 95 mL — roughly a third of normal (Chan et al., Hong Kong Med J, 2022).
This condition, called ketamine-associated uropathy, happens because ketamine and its breakdown products in urine directly damage the bladder lining. The lining erodes, inflammation sets in, and the bladder wall thickens with scar tissue. In severe cases, 30% of chronic users develop hydronephrosis — where urine backs up into the kidneys — which can lead to kidney failure. Some people end up needing surgical bladder reconstruction. The damage typically stops progressing when ketamine use stops, but existing damage may be permanent.
The cognitive effects are subtler but real. Heavy, regular ketamine use is associated with measurable impairments in working memory and episodic memory (your ability to remember events and experiences). A comprehensive review in Addiction found that these memory deficits are most pronounced in daily or near-daily users and can persist even after stopping use (Morgan & Curran, Addiction, 2012). Regular users also score higher on measures of dissociation and paranoid thinking even when not under the influence of the drug.
| System Affected | What Happens | Reversible? |
|---|---|---|
| Bladder | Inflammation, shrinkage, frequency (needing to urinate 30+ times/day), severe pain | Partially — stops progressing with abstinence, but scar tissue may be permanent |
| Kidneys | Hydronephrosis (urine backflow), possible kidney failure in severe cases | Depends on severity — some damage is permanent |
| Memory | Working and episodic memory impairment, difficulty concentrating | Partial recovery after stopping — some deficits may persist |
| Mental health | Increased dissociation, paranoid thinking, depression and anxiety | Generally improves with sustained abstinence |
| Liver | Liver damage, abnormal liver function tests | Usually reversible with abstinence |

Can You Get Addicted to Ketamine?
Yes. Ketamine produces brain changes consistent with addictive drugs, and regular users commonly develop tolerance (needing more for the same effect), compulsive use patterns, and difficulty stopping despite wanting to. Research shows that frequent users report a mean six-fold increase in dosage from their first use to their current use — meaning someone who started with 50 mg might now need 300 mg for a similar effect (Muetzelfeldt et al., Drug Alcohol Depend, 2008).
Ketamine dependence looks different from opioid or alcohol dependence. The physical withdrawal isn’t as dramatic — there’s no risk of seizures or life-threatening complications. But the psychological pull is strong. Users describe cravings, irritability, anxiety, and difficulty sleeping when they stop. Many report a pattern of using until their supply runs out, then immediately seeking more.
What makes ketamine addiction particularly tricky is that there’s no approved medication for treating it. Unlike opioid dependence (where methadone or buprenorphine can help) or alcohol dependence (where naltrexone is an option), ketamine use disorder has almost no pharmacological research behind it. Treatment relies on structured therapy — cognitive behavioural approaches (CBT), motivational interviewing, and residential programmes that remove the person from their using environment.

What Does Ketamine Treatment Look Like at One Step?
Ketamine treatment at One Step follows the same structured residential format as our other drug treatment programmes, with adjustments for ketamine-specific issues. Most clients stay 28–60 days. The programme runs on a fixed daily schedule — wake at 7am, morning meditation, breakfast at 8, group therapy from 9 to 11, individual sessions in the afternoon, and structured evening activities.
Because ketamine withdrawal isn’t medically dangerous in the way alcohol or benzodiazepine withdrawal can be, detox focuses on managing the psychological symptoms — cravings, sleep disruption, irritability, and low mood. Our visiting psychiatrist assesses each client on intake and monitors progress throughout the stay, adjusting support as needed. We don’t automatically prescribe medication, but it’s available if clinically warranted.
For clients with bladder or urinary symptoms from ketamine use, we coordinate with local medical facilities for assessment. The most important intervention for ketamine-related bladder damage is sustained abstinence — which a residential setting provides by default. Many clients notice significant improvement in urinary symptoms within their first few weeks.
The therapy side focuses heavily on what’s driving the use. Ketamine users we see tend to fall into two groups: party users whose recreational use escalated, and people who started using ketamine to self-medicate anxiety, depression, or trauma. The treatment approach differs — the first group needs relapse prevention skills and lifestyle restructuring, while the second needs the underlying issue addressed alongside the substance use.
The cost is ฿280,000/month (~$8,500 USD), which covers accommodation, all therapy sessions (group and individual), the intake assessment and routine progress checks with our visiting psychiatrist, meals, and activities. Medication, if the psychiatrist prescribes any, is billed separately — same category as flights, visas, and personal items. Aftercare planning starts in the final week, with ongoing support available after discharge.
Frequently Asked Questions About Ketamine
Common questions about how ketamine feels, its risks, and getting help.
When snorted, ketamine effects typically last 45–90 minutes, with the peak occurring within the first 20–30 minutes. When injected, effects are stronger but shorter — usually 15–60 minutes. Residual grogginess, confusion, and impaired coordination can last several hours beyond the main effects.
Fatal ketamine overdose from the drug alone is rare, but deaths do occur — usually from respiratory depression, aspiration of vomit, or accidents while incapacitated. The risk increases dramatically when ketamine is mixed with alcohol, opioids, or GHB. These combinations suppress breathing and reduce consciousness to dangerous levels.
Each drug carries different risks. Ketamine is less likely to cause acute cardiac events than cocaine, but regular ketamine use causes severe bladder damage that cocaine and MDMA don’t. Ketamine also builds tolerance faster than most recreational drugs — users commonly need six times their starting dose within months of regular use.
Ketamine withdrawal is primarily psychological, not physical. People report intense cravings, anxiety, irritability, difficulty sleeping, depression, and feeling emotionally flat. Unlike alcohol or benzodiazepine withdrawal, it’s not medically dangerous — but the psychological symptoms can be severe enough to make quitting without support very difficult.
It depends on severity. Mild to moderate bladder symptoms often improve significantly within weeks to months of stopping ketamine. But severe cases — where the bladder has shrunk, scarred, or where urine has backed up into the kidneys — may cause permanent damage. Some people require surgical bladder reconstruction. The sooner you stop, the better the chance of recovery.
Warning signs include needing more ketamine to get the same effect, using alone rather than socially, continuing despite bladder problems or memory issues, spending significant money on ketamine, and failing to cut down when you’ve tried. If any of these apply, a conversation with an addiction professional is worth having — even if you’re not sure it’s “bad enough.”
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








