
Key Takeaways
- Cocaine comes in two chemical forms: the hydrochloride salt (water-soluble powder) and the free base (a rock or paste used for smoking).
- Powder cocaine is snorted or injected; crack and traditional freebase are the same base chemistry processed for smoking.
- Smoked crack reaches the brain in seconds — that speed, plus a 5–10 minute high, is what drives compulsive binge use.
- Street cocaine averaged around 40% adulterants in international forensic samples, and the North American supply is increasingly contaminated with fentanyl.
- Cocaine does not cause the life-threatening physical withdrawal of alcohol or benzos — it causes intense psychological crash, cravings, and depression that residential treatment is built to interrupt.
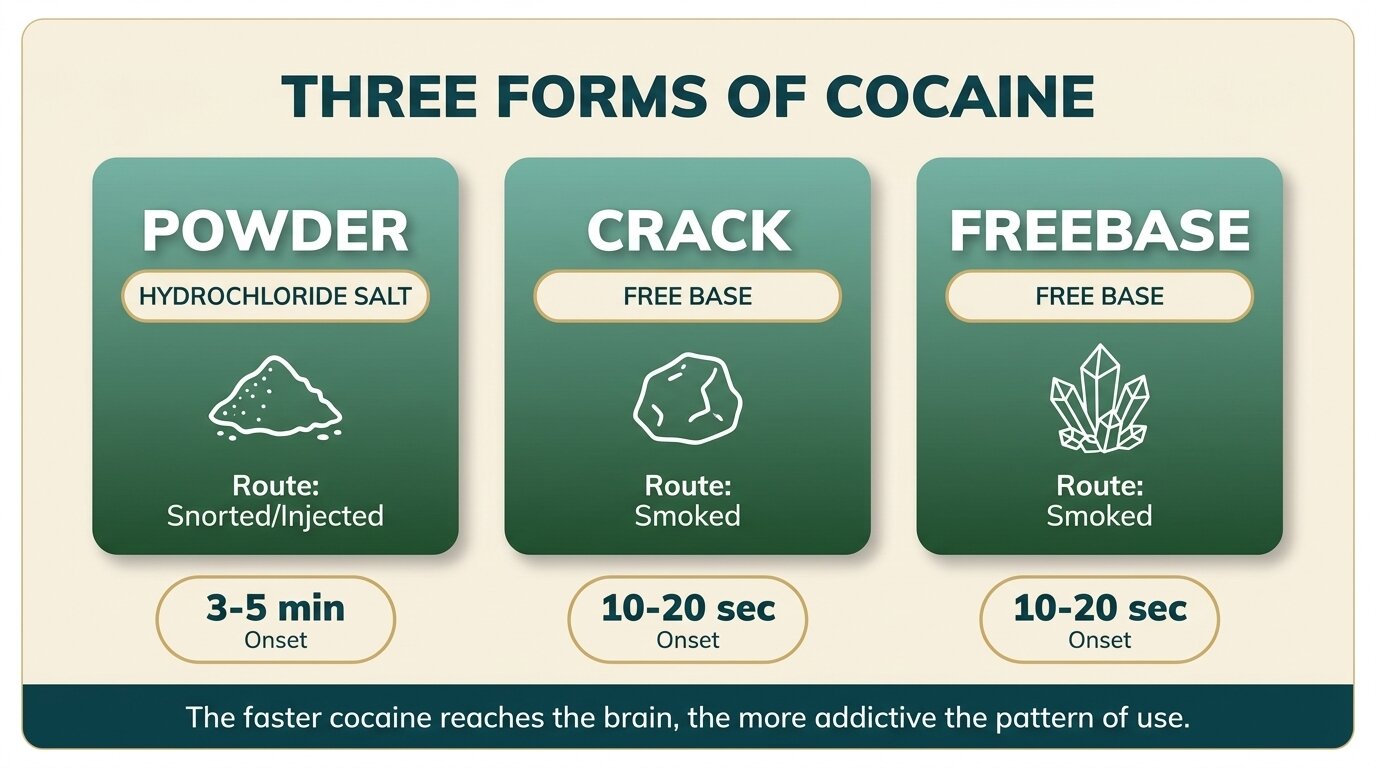
Cocaine comes in two chemical forms — the hydrochloride salt and the free base — and the form changes almost everything about how the drug behaves. Powder cocaine (hydrochloride) dissolves in water and is snorted or injected. Crack and traditional freebase are the same molecule converted into a smokable base. The chemistry sounds technical, but the practical difference is brutal: smoking cocaine delivers the drug to the brain in seconds and produces a high that collapses fast enough to drive a binge (Bravo et al., Toxins, 2022).
What are the main types of cocaine?
Cocaine has two chemical forms: the hydrochloride salt, sold as a white crystalline powder, and the free base, sold as off-white rocks (crack) or yellowish chunks (traditional freebase). The powder is water-soluble and absorbed through nasal tissue or directly into the bloodstream. Both base forms are insoluble in water but vaporise when heated — that’s what makes them smokable, and that’s what makes them more dangerous.
Every form starts from the same coca leaf extract. The “type” of cocaine comes down to how that base material is processed for sale.
- Powder cocaine — the base is reacted with hydrochloric acid to create a water-soluble salt. This is the white powder most people picture when they hear the word cocaine.
- Crack cocaine — powder cocaine is dissolved in water with sodium bicarbonate (baking soda), heated, and dried into hard rocks. The name comes from the crackling sound the rock makes when smoked.
- Freebase cocaine — the older, riskier predecessor to crack. Powder is dissolved in water and a strong base (ammonia), then extracted with a solvent like ether. The result is purer than crack but the production process has been responsible for fires and explosions.
- Coca paste (pasta base) — a crude intermediate, smoked mostly in parts of South America. Often contains kerosene, sulphuric acid, and other production residues.
How does powder cocaine differ from crack and freebase?
Powder cocaine is the hydrochloride salt — water-soluble, suitable for snorting or injecting after dissolving. Crack and freebase are both the base form — water-insoluble, designed to be smoked. The active drug is identical; what changes is how fast it reaches the brain, how long the effect lasts, and how addictive the use pattern becomes.
| Property | Powder cocaine | Crack cocaine | Traditional freebase |
|---|---|---|---|
| Chemical form | Hydrochloride salt | Free base | Free base |
| Water-soluble | Yes | No | No |
| Typical route | Snorted, injected (dissolved) | Smoked in a pipe | Smoked in a pipe |
| Time to brain | 3–5 min (snorted); ~20 sec (IV) | ~10–20 seconds | ~10–20 seconds |
| Duration of high | 20–40 minutes | 5–10 minutes | 5–10 minutes |
| Production | Coca paste + hydrochloric acid | Powder + baking soda + heat | Powder + ammonia + ether |
| Common appearance | Fine white crystalline powder | Off-white or beige rocks | Yellowish chunks or crystals |
Injecting powder cocaine reaches the brain almost as fast as smoking crack and produces a similar intensity — which is why injected cocaine carries comparable addiction risk to crack despite being the “powder” form. The route of administration, not the street name, is what predicts how dangerous a pattern of use will become. People who would never touch a crack pipe sometimes assume powder is the safer option; injected powder cocaine is not.
Why is crack cocaine more addictive than powder cocaine?
Crack hits the brain in under twenty seconds and the high collapses within ten minutes, creating an intense crash that pulls users back to the pipe almost immediately. Snorted powder cocaine takes several minutes to peak and tapers over half an hour or more, producing a milder cycle. Faster onset plus shorter duration is the formula for binge use — and binge use is the strongest behavioural predictor of cocaine dependence.
A foundational pharmacokinetic study found that smoked and intravenous cocaine both reach peak plasma concentrations within about 5 minutes, while intranasal cocaine takes around 50 minutes to peak. Behavioural effects, however, were substantially higher with smoked administration than with intravenous administration at equivalent doses — meaning the smoked route does something to the brain that injection alone doesn’t replicate (Cone, Journal of Analytical Toxicology, 1995).
The practical consequence: someone who smokes crack rarely smokes once. The binge pattern is structural, not a failure of willpower. We see people walk into cocaine rehab describing two-day, three-day, sometimes week-long sessions where the only stop is when the supply or the money runs out. That’s the form doing the talking, not the user.
What people don’t always understand about crack is that the speed of the high is also the speed of the crash. The faster a drug arrives, the faster the brain demands more of it. Powder cocaine is dangerous, but the smokable forms compress an entire addiction cycle into a single afternoon.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
What’s actually in street cocaine?
Street cocaine is rarely sold pure. Forensic analyses of seized samples have found average purity well under 60%, with the rest made up of cutting agents, manufacturing residues, and increasingly other psychoactive drugs. Adulterants are mixed in to stretch supply, mimic cocaine’s local-anaesthetic numbing effect, or amplify the perceived stimulant rush.
Common adulterants documented in international forensic literature include (Bravo et al., Toxins, 2022):
- Inert bulking agents — talc, cornstarch, sugar, flour. Cheap, visually plausible, biologically inert (though injected talc can cause lung damage).
- Local anaesthetics — procaine, lidocaine, benzocaine. Replicate cocaine’s numbing effect on the gums or nose, helping a low-purity sample “test” believable.
- Other stimulants — caffeine, amphetamines, ephedrine. Mimic or amplify the rush without contributing real cocaine.
- Levamisole — a veterinary deworming agent found in a high proportion of cocaine samples across North America and Europe. Linked to immune-system suppression and skin necrosis with chronic use.
- Fentanyl and synthetic opioids — the highest-risk contemporary contaminant. Increasingly present in North American cocaine and crack supplies, driving cocaine-involved overdose deaths that look like opioid overdoses on autopsy.
The fentanyl problem is the reason cocaine-involved overdose deaths in the United States rose sharply through 2023 — 29,449 deaths that year — before declining to 21,945 in 2024 alongside the broader downturn in opioid mortality (Garnett & Miniño, NCHS Data Brief No. 549, 2026). A bag of “cocaine” in 2026 is a chemistry problem, not a known quantity.

How quickly does each form take effect?
The route of administration sets the timeline. Smoked crack and traditional freebase reach the brain in roughly 10–20 seconds because the lungs deliver the drug straight into pulmonary circulation. Snorted powder cocaine takes 3–5 minutes to begin and 20 minutes or more to peak. Injected powder is comparable to smoking in speed but lasts somewhat longer per dose. The slower the onset, the gentler the eventual crash.
| Route | Form used | Onset | Peak effect | Duration |
|---|---|---|---|---|
| Smoked | Crack or freebase | ~10–20 seconds | 1–3 minutes | 5–10 minutes |
| Injected | Powder (dissolved) | ~20–30 seconds | 3–5 minutes | 15–30 minutes |
| Snorted | Powder | 3–5 minutes | ~20 minutes | 20–40 minutes |
| Oral / gummed | Powder | 10–30 minutes | ~60 minutes | 30–60 minutes |
People often present themselves to treatment categorising their use by the substance (“I have a cocaine problem”), but during assessment the route tells us far more about severity and prognosis. A daily smoker faces a different recovery curve than a weekend snorter, even at similar gram-per-week totals.
Trying to work out whether your use has crossed the line? Talk to our team — we’ll give you a straight answer about whether residential treatment is the right step.
What are the long-term health risks of each form?
Long-term cocaine use damages the cardiovascular system regardless of the form — heart attack, stroke, and arrhythmias are documented at any route. The form, however, determines what other organs take the brunt. Snorting destroys nasal tissue; smoking damages the lungs and dental structure; injecting introduces blood-borne disease risk and vein damage. The differences matter for medical screening on intake.
| Form & route | Risks unique to this route |
|---|---|
| Snorted powder | Perforated nasal septum, chronic sinusitis, loss of smell, palate erosion |
| Injected powder | HIV, hepatitis B and C, endocarditis, abscesses, deep-vein thrombosis |
| Smoked crack / freebase | “Crack lung” (acute pulmonary haemorrhage), chronic bronchitis, severe dental decay, burns to lips and fingers |
| All forms | Heart attack, stroke, arrhythmia, seizures, paranoia, depression, cocaine-induced psychosis |
Cocaine does not cause the life-threatening physical withdrawal that alcohol or benzodiazepines do. There’s no seizure risk during a cocaine “detox.” What it does cause is a severe psychological crash — exhaustion, depression, anhedonia, intense cravings — that typically peaks in the first week and gradually eases over several weeks. The lack of a dramatic medical withdrawal is exactly why people convince themselves they can quit alone, and exactly why that approach so reliably ends in relapse.

What does cocaine treatment look like at One Step Rehab?
At One Step we treat cocaine addiction across all three forms — powder, crack, and injected — on-site as a standard inpatient case. There’s no medical withdrawal to manage in an ICU sense, so the work is psychological from day one: structured group therapy, individual CBT and DBT sessions, supervised abstinence, and the kind of distance from triggers that almost no home environment can provide.
Specifics worth knowing before you enquire:
- Programme length: Most cocaine clients stay 28–60 days. Shorter than 28 is rarely enough time for the psychological crash to fully resolve. Our treatment programme page lays out the structure.
- Cost: ฿280,000 per month (roughly USD 8,500). The full inclusion and exclusion list is on our pricing page. Medication, flights, visa fees, and personal items are billed separately — like any inpatient rehab.
- Daily structure: Wake at 7am, group therapy mid-morning, one-to-one counselling, afternoon physical activity, evening reflection. The treatment schedule shows a typical week.
- Setting: Mid-range residential in Chiang Mai. Not luxury — no infinity pool, no private chef. The investment goes into clinical time, not amenities.
- Aftercare: The first 90 days after discharge are when cocaine clients most often relapse. Our aftercare programme provides structured continuing contact during that window; our blog on common relapse triggers covers the patterns we see repeatedly.
- Polysubstance use: Many cocaine clients also drink heavily — the combination produces cocaethylene in the liver, with its own cardiovascular risks (we cover this in our post on cocaine and alcohol). Assessment screens for this from intake.
If you or someone you love is struggling with substance dependence, explore how a professional drug addiction treatment can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Quick answers to questions people most often ask about the different types of cocaine.
No — both contain the same active molecule, cocaine. The difference is the chemical form. Powder is the hydrochloride salt; crack is the free base. The base form vaporises at lower temperatures, which is what makes it smokable. The high-risk difference is the speed of delivery to the brain, not the molecule itself.
Diagnosable dependence after a single use is rare, but a powerful psychological pull to use again is common — especially after smoking crack. Many people describe their first crack experience as creating an immediate craving for more, which is why the smokable forms drive a fast path to compulsive use even in people without prior addiction history.
Crack has largely replaced traditional freebase since the 1980s because it’s cheaper and safer to produce — baking soda instead of flammable solvents like ether. Some users still freebase from powder using kitchen methods, but the practice is much less common than smoking crack rocks bought ready-made.
Contamination is mostly cross-contamination in the supply chain rather than deliberate addition — fentanyl is so potent that microscopic residues on equipment, scales, or packaging can be enough to kill a stimulant user with no opioid tolerance. This is the primary reason cocaine-involved overdose deaths spiked in the United States from 2020 onward.
Cocaine itself has a short half-life — most is gone from blood within hours. Its main metabolite, benzoylecgonine, is what drug tests detect. Urine tests pick it up for 2–4 days after a single use and up to 10–14 days after heavy or chronic use. Hair tests can detect cocaine use for 90 days or more.
By route of administration, smoked crack and injected powder carry the highest addiction risk and the highest acute overdose risk. By contamination risk, any street cocaine in regions affected by fentanyl-tainted supply is dangerous regardless of form. The “safer” snorted route still causes heart attacks, strokes, and dependence.
There is no approved medication to treat cocaine dependence the way methadone or buprenorphine treat opioid dependence. The evidence base for cocaine treatment is built around psychological work — cognitive behavioural therapy, contingency management, motivational interviewing, and structured residential abstinence. Sleep and mood medications are sometimes used short-term, but the core treatment is therapeutic.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








