
Key Takeaways
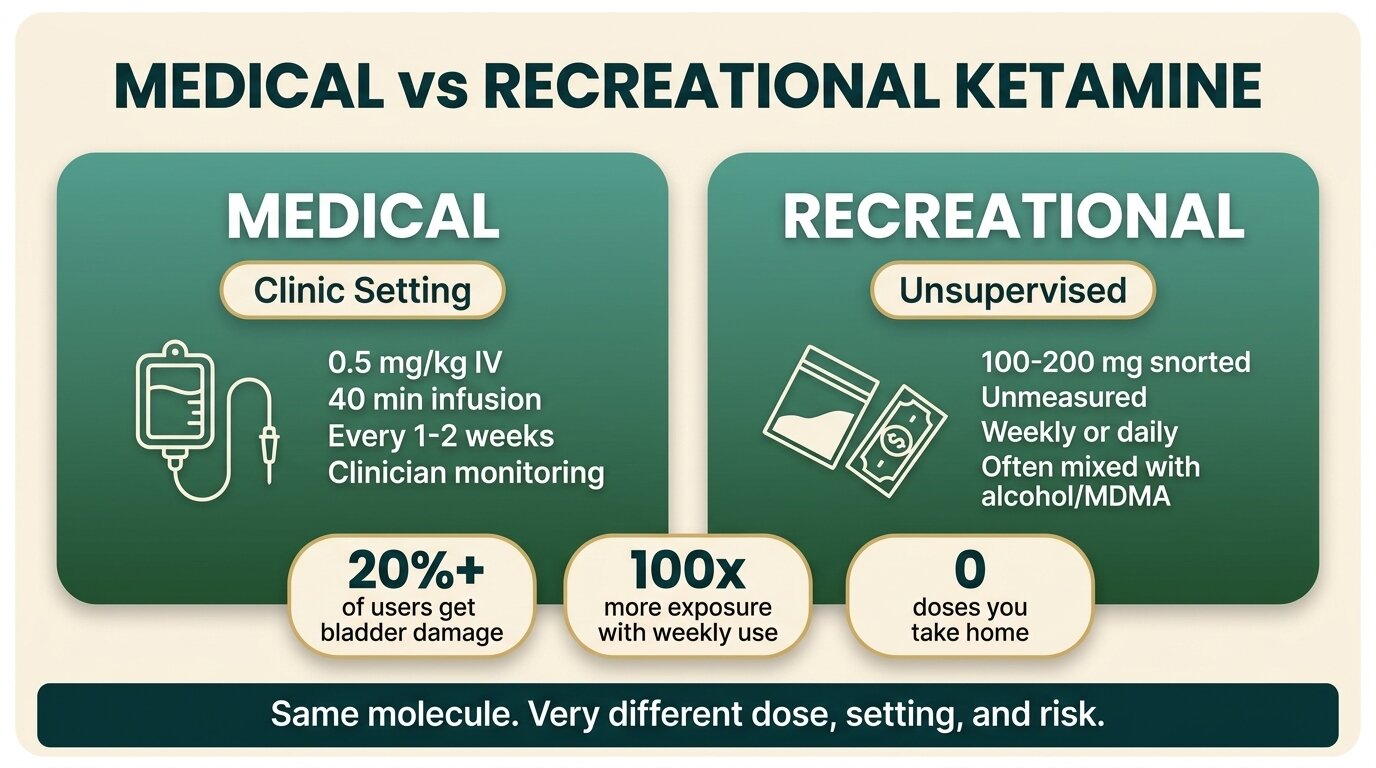
- Medical ketamine is dosed at around 0.5 mg/kg by slow IV infusion in a clinic, with vital signs monitored and a doctor present. Recreational ketamine is typically 100-200 mg snorted, unmeasured, and often combined with alcohol or MDMA.
- “Ketamine-assisted therapy” means a single supervised dose every few weeks alongside psychotherapy. It is not a prescription you take home, and it is not the same molecule used in a new setting.
- Esketamine (Spravato) is FDA-approved for treatment-resistant depression and is given in a certified clinic with a two-hour observation period — not dispensed for self-administration.
- The bladder, kidney, and memory damage seen in heavy chronic users comes from the cumulative exposure of frequent recreational use, not from a single supervised infusion every few weeks.
- FDA approval for depression does not make recreational use safe. Same molecule, very different exposure, very different risk.
Medical ketamine and recreational ketamine are the same drug used in two completely different ways. A medical infusion is around 0.5 mg/kg given slowly into a vein in a monitored clinic, then repeated every few weeks (Berman et al., Biol Psychiatry, 2000). Recreational use is roughly 100-200 mg of unmeasured powder snorted in a club, sometimes weekly, often mixed with alcohol or MDMA. The molecule is identical. The dose, the setting, and the cumulative exposure are not — and that is where the harm lives.
What Counts as Medical Ketamine Use?
Medical ketamine use means a precisely weighed dose, administered by a clinician in a setting with monitoring equipment and emergency support. For depression, the standard is 0.5 mg/kg of racemic ketamine infused intravenously over 40 minutes, repeated every 1-2 weeks (Sanacora et al., JAMA Psychiatry, 2017). The FDA-approved nasal version, esketamine (Spravato), is given in a certified clinic with two hours of observation afterwards.
What makes it “medical” is not the molecule. It is everything around the molecule: the dose calculation, the slow infusion rate, the trained clinician, the blood-pressure cuff, the controlled environment, and the long gap between sessions. A patient receiving Spravato cannot take the bottle home. They sit in a chair in a clinic, get the dose, and are watched until the dissociation wears off.
This protocol traces back to the original Berman trial at Yale, which gave seven patients with depression a single 0.5 mg/kg infusion and found rapid relief that lasted up to a week. That study became the template for every clinical ketamine programme since.

What Does Recreational Ketamine Use Look Like?
Recreational ketamine is typically 100-200 mg of unmeasured powder snorted at a club or party, often several times in one night, frequently combined with alcohol, MDMA, or cocaine (NIDA, 2024). Users buy from dealers, so purity is unknown. Doses are eyeballed with a credit card on a table. There is no clinician, no blood pressure monitor, and no observation period afterwards.
The pattern of use also differs. A medical patient receives one supervised dose every one to two weeks for a defined course. A heavy recreational user might snort key bumps every 20 minutes for an entire night, every weekend, for years. The cumulative exposure across a year of weekend use can easily reach 100 times what a medical patient receives across the same period.
Polydrug use makes the recreational pattern more dangerous. Mixing ketamine with alcohol amplifies dissociation and respiratory depression. Combining it with MDMA (sometimes called “kitty flipping”) strains the heart and raises overdose risk. Of 23 ketamine-involved deaths in the UK reviewed in one forensic series, only 4 involved ketamine alone — the other 19 involved drug combinations.
How Do the Two Compare Side by Side?
The simplest way to see the gap between medical and recreational ketamine is to put them next to each other. Dose, route, setting, frequency, and supervision differ on every dimension — even though the active ingredient is the same.
| Factor | Medical Ketamine | Recreational Ketamine |
|---|---|---|
| Typical dose | ~0.5 mg/kg (≈35 mg for a 70 kg adult) IV, or 56-84 mg esketamine nasal | 100-200 mg snorted per session, often repeated |
| Route | Slow IV infusion (40 min) or nasal spray under supervision | Snorted (insufflated), sometimes injected or swallowed |
| Frequency | Once every 1-2 weeks during induction; then maintenance every 2-4 weeks | Weekend use, sometimes daily; binge sessions with repeated dosing |
| Setting | Certified clinic with BP cuff, oxygen, trained clinician | Club, party, home; no monitoring |
| Observation after dose | Minimum 2 hours of post-dose monitoring | None |
| Combined with other drugs | Used with an oral antidepressant; no recreational mixers | Frequently mixed with alcohol, MDMA, cocaine |
| Cumulative annual exposure | Roughly 12-24 supervised doses per year | Can exceed 100x the medical exposure with weekly heavy use |
What Does “Ketamine-Assisted Therapy” Actually Mean?
Ketamine-assisted therapy is a clinical model where a supervised ketamine dose is paired with psychotherapy sessions before and after. The dose is given in a clinic, with a therapist present, and the work happens in the integration sessions that follow — not during the dissociation itself. It is not self-medication, and the patient never takes ketamine home.
The model emerged after the Berman trial showed that a single dose could produce rapid antidepressant effects. Clinicians began pairing the dose with structured therapy to extend the benefit. In a typical protocol, a patient has a preparation session, then a dosing session in a quiet room with a clinician monitoring vital signs, then one or more integration sessions where they make sense of what came up.
What it is not: an at-home prescription, a daily medication, a recreational experience with a therapist label, or a green light to buy ketamine on the street. Reputable ketamine-assisted therapy programmes screen for cardiovascular risk, bladder symptoms, prior addiction history, and active substance use before accepting a patient. The 2017 JAMA Psychiatry consensus statement was explicit that off-label use without these safeguards carries real risk.
The clearest sign someone has crossed from use into a problem is when the dose stops being a discrete event and starts becoming a daily presence — bumps to get through the morning, more in the afternoon, then heavier at night. At that point the molecule is the same molecule a depression patient gets in a clinic, but the exposure has multiplied by orders of magnitude. That’s where the bladder damage, the memory loss, and the dependency live.
Dr. Worapakthorn KongpesalaphunConsultant Psychiatrist, One Step Rehab
Worried that ketamine use has stopped being recreational? Talk to our team — we’ll give you a straight answer about whether what you’re describing needs treatment.

If Medical Ketamine Is Safe, Why Is Recreational Ketamine Still Risky?
Because the harm is in the cumulative dose, not the molecule. A patient receiving one supervised 35 mg IV dose every two weeks is exposed to roughly 900 mg of ketamine a year. A weekend recreational user snorting 400 mg every Saturday is exposed to over 20,000 mg a year. The bladder, kidneys, and brain respond to total exposure, not to whether the dose came from a clinic or a dealer.
Ketamine-induced cystitis affects more than 20% of recreational users (Anderson et al., Health Psychol Res, 2022). It starts as painful urination and frequency, progresses to reduced bladder capacity, and in severe cases requires bladder removal. Cognitive harm follows the same pattern. Frequent users showed measurable impairments in spatial and episodic memory linked to reduced hippocampal activation (Morgan et al., Front Psychiatry, 2014). A 3-year longitudinal study found that episodic memory damage persisted even after users substantially cut back (Morgan et al., Addiction, 2004).
None of this contradicts the depression evidence. The medical use is real and the bladder damage is real, and they live on the same dose-response curve. One dose every two weeks under supervision is on the safe end. Hundreds of milligrams snorted every weekend is on the harm end. The molecule does not know which end you are on.
Can You Self-Medicate Depression With Recreational Ketamine?
No. The fact that ketamine treats depression in a clinic does not transfer to street ketamine in a flat. The clinical effect depends on the dose, the route, the spacing between doses, and the therapeutic context. Repeated heavy recreational use produces the opposite of the antidepressant effect over time — including cognitive decline, urinary pain, and ketamine use disorder.
Self-medication with recreational ketamine misses three things that the clinical model has built in. First, the dose is wrong: clinics use a calculated 0.5 mg/kg, not 200 mg eyeballed. Second, the frequency is wrong: clinics space doses by 1-2 weeks to avoid tolerance and bladder damage. Third, the therapy is missing: the antidepressant benefit in trials was measured in patients receiving structured care, not in solo home users with a bag of K.
The pattern we see in residential treatment is consistent. People who started using ketamine to “treat” depression often arrive years later with chronic bladder pain, memory complaints, and a depression that is now worse than when they started — because the chronic use has compounded the original mood problem with new physical and cognitive damage.

How Does One Step Treat Ketamine Addiction?
One Step runs a 28-60 day residential programme in Chiang Mai for clients with ketamine dependence. Detox from ketamine is handled on-site — there is no severe physical withdrawal syndrome the way there is with alcohol or benzodiazepines, so the focus is on managing cravings, sleep disturbance, and the psychological pull back to use. The programme costs approximately ฿280,000/month (~$8,500 USD).
What’s included in the fee: accommodation, three daily meals, the full structured treatment programme, group and individual therapy, intake assessment with our visiting psychiatrist, and activities and excursions built into the weekly schedule. What’s not included: prescribed medication, flights, visas, and personal items. Any medication our visiting psychiatrist prescribes during your stay is billed separately. See the pricing page for the full breakdown.
For clients arriving with ketamine-induced bladder damage, we work with local urology services for assessment and pain management while the rehab programme runs in parallel. Cessation of ketamine use is associated with symptom improvement in most cases, which is one reason the residential model works — you are out of the environment where the drug was easy to access.
Our clinical model uses CBT and DBT alongside the therapeutic community model. For the ketamine cluster specifically, our work covers the dissociation pattern, the polydrug context (most clients used ketamine with other substances), and rebuilding cognitive function after heavy use. The ketamine rehab programme page has the full clinical detail. Background reading on the experience itself: how ketamine actually feels and the K-hole.
If you or someone you love is struggling with substance dependence, explore how a drug addiction treatment programme can provide the structure, clinical support, and environment needed for lasting recovery.
Frequently Asked Questions
Common questions about how medical and recreational ketamine differ.
The molecule is identical, but everything else differs. Ketamine therapy uses a calculated dose (around 0.5 mg/kg IV or 56-84 mg nasal esketamine) given in a clinic with monitoring and a two-hour observation period. Recreational use is unmeasured powder snorted without supervision, often combined with other drugs. Same drug, very different exposure and risk.
Bladder and kidney damage from ketamine is dose-dependent. A medical patient receives one supervised dose every 1-2 weeks. A heavy recreational user can snort the equivalent of dozens of medical doses in a single weekend. The cumulative exposure is what damages the urinary tract, not the molecule itself.
No. Spravato (esketamine) can only be administered in a certified clinic under direct supervision, with at least two hours of post-dose observation. It is not dispensed for self-administration. This is part of the FDA’s Risk Evaluation and Mitigation Strategy programme designed to prevent diversion and misuse.
Yes. Heavy recreational ketamine use can produce psychological dependence, tolerance, and a withdrawal pattern dominated by cravings, low mood, anxiety, and sleep disturbance. The risk increases with frequency of use. See our page on ketamine rehab for treatment options.
Yes. Alcohol amplifies ketamine’s dissociation and respiratory depression. MDMA combined with ketamine strains the cardiovascular system and raises overdose risk. Most recorded ketamine-involved deaths involve other substances, not ketamine alone. Polydrug use is the most dangerous part of the recreational pattern.
Partly. Semantic memory tends to recover after substantial reduction in use. Episodic memory impairment — the ability to recall specific events — appears more persistent in longitudinal studies. The earlier someone stops, the better the recovery. Memory problems should not be dismissed as something that will “just clear up” without abstinence.
No. The depression evidence applies to a specific clinical protocol (one supervised dose every 1-2 weeks, alongside therapy), not to weekend recreational use. Self-medicating with street ketamine tends to worsen mood over time, adds the risk of bladder and cognitive damage, and can develop into dependency. If depression is the underlying problem, treat the depression with a clinician.
Written by
Worapakthorn Kongpesalaphun, MD., Ph.D.
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Worapakthorn








