Key Takeaways
- Inpatient rehab means living at the facility full-time with structured daily support, therapy, and separation from triggers. Outpatient means attending sessions a few hours per week while living at home — a fundamentally different level of care.
- For severe addiction, medically dangerous withdrawal (alcohol, benzodiazepines, opioids), co-occurring mental health conditions, or failed outpatient attempts, inpatient treatment is significantly safer and more effective.
- At One Step, your day is structured from 7am to 9pm: group therapy every morning, individual counselling weekly, Muay Thai or gym in the afternoon, recovery meetings in the evening. There’s no unsupervised downtime in the first week.
- Outpatient rehab works best as a step-down after completing residential treatment — not as a starting point for serious addiction. The relapse risk during early recovery is too high without residential structure.
- One Step only offers inpatient treatment. We’ve seen too many clients arrive after failed outpatient attempts to believe that serious addiction can be treated in evening sessions.
Inpatient rehab works better than outpatient for serious addiction. That’s not a sales pitch — it’s what the evidence consistently shows. NIDA identifies residential treatment as most appropriate for people with severe substance use disorders, particularly when co-occurring mental health conditions or unstable home environments are involved (CADTH Health Technology Review).
One Step only offers inpatient treatment. We made that decision because the clients who reach us — often after failed outpatient attempts — need full-time structure, medical oversight during detox, and complete separation from their using environment. Outpatient has its place, but it’s rarely the right starting point for someone whose addiction has reached the point where they’re researching rehab in Thailand.
This post breaks down the real differences between inpatient and outpatient, when each approach makes sense, and what residential treatment actually looks like day-to-day at One Step.
What Is the Difference Between Inpatient and Outpatient Rehab?
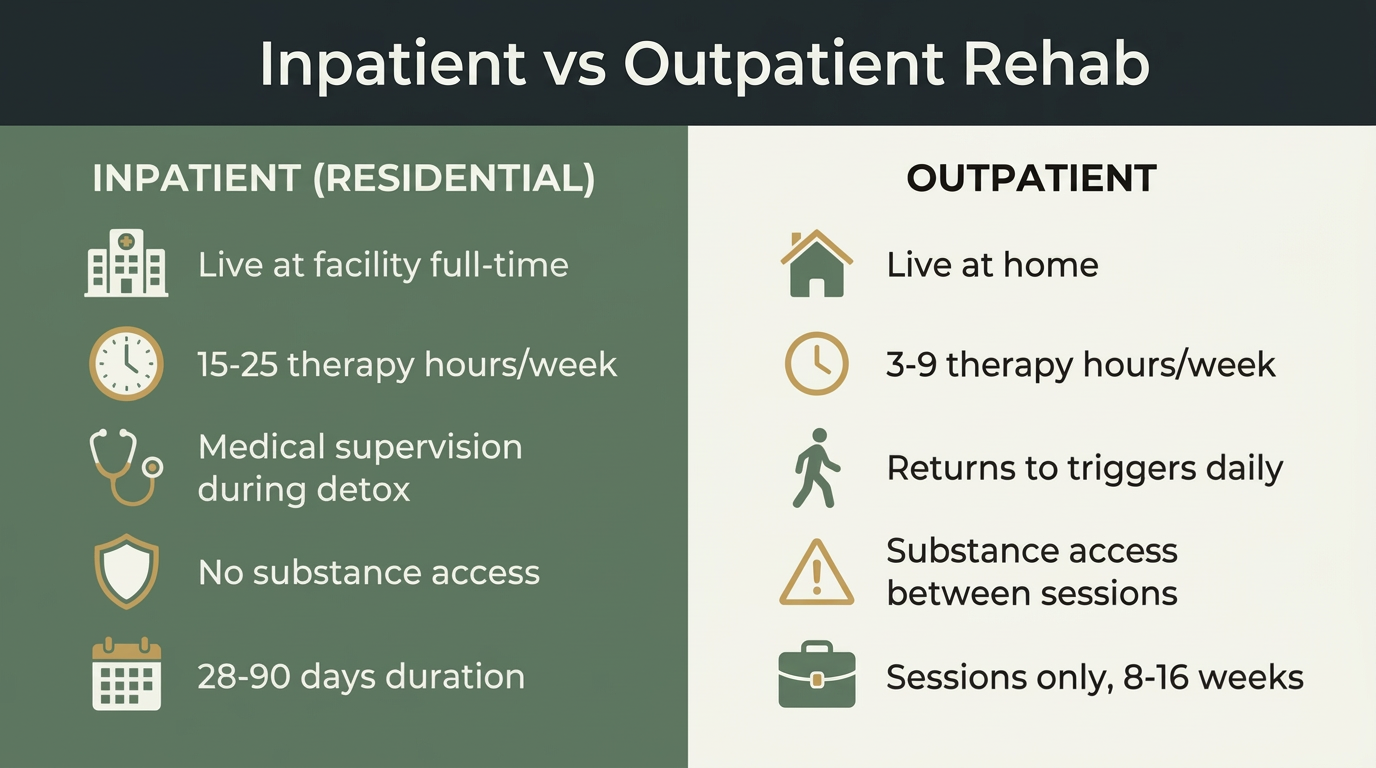
Inpatient rehab requires you to live at the treatment facility full-time for 28–90 days, with structured therapy, medical supervision, and no unsupervised access to substances. Outpatient rehab lets you attend scheduled therapy sessions — typically a few hours per week — while continuing to live at home and maintain daily responsibilities.
The difference isn’t just logistical. It changes the intensity of care, the safety during withdrawal, and how much of your day is devoted to recovery versus the environment that contributed to your addiction.
| Factor | Inpatient (Residential) | Outpatient |
|---|---|---|
| Where you live | At the facility, full-time | At home |
| Therapy hours/week | 15–25 hours (One Step: ~20 hrs) | 3–9 hours |
| Medical supervision | Regular check-ins during detox, ongoing oversight after | Scheduled appointments only |
| Substance access | None — controlled environment | Full access between sessions |
| Trigger exposure | Removed from triggers entirely | Returns to triggers daily |
| Best for | Severe addiction, dangerous withdrawal, dual diagnosis, failed prior treatment | Mild substance use, step-down after residential, strong home support |
| Typical duration | 28–90 days | 8–16 weeks (sessions only) |
| Cost (Thailand) | ฿280,000/month (~$8,500 USD) at One Step | Not widely available in Chiang Mai |
What About the Middle Ground — IOP and PHP?
Inpatient and outpatient aren’t the only two options. In many countries, two middle-ground programmes exist:
- Partial Hospitalisation Programme (PHP) — 5–6 hours of treatment per day, 5 days a week. You attend the facility during the day but go home in the evening. Appropriate for people who need intensive support but have a stable, substance-free home to return to.
- Intensive Outpatient Programme (IOP) — 3–4 hours per day, 3–5 days per week. Less intensive than PHP but significantly more structured than standard outpatient. Often used as a step-down from residential treatment.
| Level | Hours/week | Where you live | Best for |
|---|---|---|---|
| Inpatient (residential) | 15–25+ structured hours | At the facility | Severe addiction, dangerous withdrawal, co-occurring disorders |
| PHP | 25–30 hours | At home (stable environment required) | Moderate addiction with safe home, step-down from inpatient |
| IOP | 9–20 hours | At home | Step-down after residential, moderate use with support |
| Standard outpatient | 1–3 hours | At home | Mild use, maintenance, long-term follow-up |
In Thailand, PHP and IOP programmes are not widely available — the treatment landscape is primarily residential or outpatient. One Step only offers residential treatment because the clients who travel to Thailand for rehab have typically exhausted local options and need the intensity and separation that only inpatient care provides.
At One Step, the therapy total comes to roughly 20 structured hours per week: daily group therapy (CBT-focused), weekly individual counselling, plus fitness sessions, meditation, and recovery meetings. That’s roughly triple what even intensive outpatient programmes deliver — and it happens in an environment where substances simply aren’t available.
However, at One Step Rehab, we do offer a “step-down programme” during the third month where clients continue to live on site but go out in pairs during the day. During that step-down period, our clients self-manage to a greater degree and arrange their own daily activities including accessing 12-step support groups in Chiang Mai city. Upon return to our centre, they are urine tested to ensure accountability. We find that this prepares our clients for their return to the “real world” when they get home.

When Does Inpatient Rehab Make More Sense Than Outpatient?
Inpatient treatment is the better choice when addiction is severe, when withdrawal is medically dangerous (alcohol, benzodiazepines, opioids), when previous outpatient attempts have failed, when co-occurring mental health conditions need simultaneous treatment, or when the home environment contains active triggers that make early recovery unsafe.
The American Society of Addiction Medicine’s ASAM guidelines recommend residential care when any of the following apply:
- Medically dangerous withdrawal. Alcohol and benzodiazepine withdrawal can cause seizures and be life-threatening. This requires close medical monitoring — not a weekly check-in. At One Step, detox is medically supervised for the first 3–7 days with staff support on site.
- Failed outpatient treatment. Most of our clients have tried outpatient first. It didn’t work — not because the therapy was bad, but because they went back to the same environment, the same people, and the same access to substances every evening.
- Co-occurring mental health conditions. Depression, anxiety, PTSD, or bipolar disorder alongside addiction requires coordinated treatment. At One Step, dual diagnosis is managed by Dr. Worapakthorn, our consulting psychiatrist, who can adjust medications and monitor interactions in real time.
- Unstable home environment. If your household includes active substance use, enabling relationships, or domestic instability, outpatient treatment is fighting against your own living situation.
- Severe addiction with high daily use. Heavy daily use of alcohol, methamphetamine, opioids, or cocaine typically requires the intensity of residential treatment to break the cycle.

What Happens During Inpatient Treatment at One Step?
At One Step, inpatient treatment follows a structured daily programme: group therapy every morning, individual counselling weekly, physical fitness (Muay Thai, gym, swimming) in the afternoon, and recovery meetings in the evening. Detox is medically supervised for the first 3–7 days, with psychiatric oversight from Dr. Worapakthorn for clients with dual diagnosis.
Here’s what a typical day looks like — not a brochure version, the actual treatment schedule:
- 7:00am — Wake up, optional morning meditation
- 8:00am — Breakfast (high-protein, dopamine-supporting meals)
- 9:00–10:00am — Muay Thai, swimming, weightlifting, cycling, or yoga
- 10:30am–12:00pm — Group therapy (CBT-based, rotating topics)
- 12:00–1:00pm — Lunch
- 2:00–3:00pm — Individual counselling or specialist session (TRE, trauma work)
- 3:00–4:00pm — Therapeutic Thai massage
- 4:00–5:00pm — Holistic therapy groups (mantra practice, Vipassana meditation, breathwork, sound therapy)
- 6:00pm — Dinner
- 7:30pm — Recovery meeting or group reflection
- 9:00pm — Quiet time, lights out by 10:30pm
The first week is the most structured. Clients coming off substances have limited unsupervised time, phone access is restricted, and medical check-ins happen multiple times daily during detox. This isn’t punitive — it’s protective. The first 72 hours of alcohol or benzo withdrawal are when medical emergencies happen, and the first week is when most outpatient clients relapse.
After the initial stabilisation period, the programme opens up. During month one, clients complete their mind maps and life story. During month two, they investigate their triggers through CBT exercises and psycho-education. During the third month, clients are able to gain more autonomy via our “Step Down” programme. Clients are able to leave the site during the day, which slowly exposes them to triggers in manageable doses while still residing at the centre. We find that this helps clients to shift the focus from crisis management to building the habits, coping strategies, and self-awareness that sustain recovery after discharge.
Every client gets a personalised treatment programme based on their intake assessment. Substance type, severity, mental health history, and personal goals all shape which therapies are emphasised. We don’t run a one-size-fits-all conveyor belt.

What Are the Limitations of Outpatient Rehab?
Outpatient rehab’s primary limitation is that clients return to their using environment after every session. Without full-time structure and supervision, people in early recovery face constant exposure to triggers, substances, and social pressures that make relapse significantly more likely — particularly in the first 30 days when cravings peak.
Research published in the Journal of Substance Abuse Treatment found that patients in residential treatment had significantly higher completion rates and lower relapse rates in the first 90 days compared to outpatient participants, particularly those with severe substance use disorders (GJ Stahler et al., Addict Behav. 2016).
That said, outpatient isn’t useless. It works well in two scenarios:
- As a step-down after inpatient. Completing 28–60 days of residential treatment, then transitioning to outpatient sessions at home, is the evidence-supported approach. This is what our step-down programme and free 12-month aftercare programme are designed to do.
- For mild substance use with strong support. Someone with a manageable drinking problem, a stable home, a supportive family, and no co-occurring mental health issues may genuinely do well with outpatient therapy. But that’s a narrow profile — and it’s not the typical person searching for rehab in Thailand.
One Step doesn’t offer outpatient because we don’t think it serves our client base well. The people who contact us have usually already tried managing their addiction while maintaining their normal life. It didn’t work. They need a reset — not more evening appointments.
What Do the Numbers Actually Show?
The data consistently favours residential treatment for severe addiction. A large-scale analysis published in the Journal of Substance Abuse Treatment found that inpatient programme completion rates average around 65%, compared to approximately 52% for outpatient — and completion is the single strongest predictor of long-term sobriety (Gerald J Stahler et al., Addict Behav. 2016).
But the numbers need context. Success rates depend heavily on:
- Length of stay. NIDA data shows that treatment lasting at least 90 days produces significantly better outcomes regardless of setting. A 7-day detox-only stay isn’t comparable to a 60-day residential programme.
- Aftercare engagement. Clients who engage in structured aftercare after residential treatment have markedly lower relapse rates. The residential stay builds the foundation; aftercare maintains it.
- Severity of addiction. Outpatient can match inpatient outcomes for mild-to-moderate substance use with strong home support. For severe addiction, inpatient consistently outperforms.
- Co-occurring disorders. Dual diagnosis clients (addiction + depression, anxiety, PTSD) show significantly better outcomes in residential settings where both conditions are treated simultaneously.
The strongest model isn’t “inpatient OR outpatient” — it’s a continuum. Start with residential to stabilise, detox, and build coping skills in a controlled environment. Then step down to IOP or regular outpatient therapy at home. This sequential approach, which One Step’s step-down and aftercare programme is specifically designed to support, produces the best long-term outcomes.
How Do You Decide What Level of Care You Need?
If you’re unsure whether inpatient treatment is necessary, work through these questions honestly:
- Is withdrawal medically risky? If you’re a daily heavy drinker, use benzodiazepines, or have a history of withdrawal seizures → inpatient with medical supervision is non-negotiable.
- Have you tried outpatient or self-directed approaches before? If they didn’t work, repeating the same approach is unlikely to produce different results. Inpatient provides the structural change you need.
- Is your home environment stable and supportive? If your partner drinks, substances are easily accessible, or your household is chaotic → inpatient removes you from those triggers entirely.
- Do you have co-occurring mental health conditions? Depression, anxiety, PTSD, or ADHD alongside addiction requires coordinated treatment that’s extremely difficult to deliver in 1-hour weekly sessions.
- Can you take 28–60 days away from responsibilities? This is the practical constraint. If you genuinely cannot take leave from work or caregiving, IOP may be a workable compromise — but be honest about whether “can’t” means “can’t” or “don’t want to.”
If you answered “yes” to questions 1–4, inpatient is almost certainly the right starting point. If your situation is milder and your support system is strong, outpatient or IOP may be sufficient — but consider inpatient if previous attempts haven’t stuck.
Common Misconceptions About Rehab
“Inpatient is always better.” Not necessarily. For mild substance use with a stable home and strong social support, outpatient can produce equivalent outcomes. The key is matching the level of care to the severity of the problem.
“Outpatient is just for mild cases.” Modern IOP and PHP programmes are clinically rigorous — 15–30 hours of therapy per week with medication management and trauma-informed care. They’re not “diet rehab.”
“Rehab is 28 days and you’re cured.” Addiction is a chronic condition. The 28-day programme builds the foundation. Recovery is maintained through ongoing aftercare, peer support, lifestyle changes, and continued therapy — potentially for years.
“If you relapse, treatment failed.” Relapse rates for addiction (40–60%) are comparable to relapse rates for other chronic conditions like diabetes and hypertension. A relapse doesn’t mean treatment was useless — it means your recovery programme needs to be strengthened.
“You have to hit rock bottom.” This is the most dangerous misconception. Early intervention produces significantly better outcomes. The longer you wait, the more damage addiction does to your brain, body, relationships, and career — and the harder recovery becomes.
The first 30 days of recovery are when the brain is most vulnerable to relapse. Withdrawal symptoms, disrupted sleep, and intense cravings all peak during this period. In a residential setting, we can manage those risks in real time — adjusting medications, providing immediate therapeutic support, and keeping the client in a substance-free environment. In outpatient, the client goes home after their session and faces all of those challenges alone. For severe addiction, that’s asking too much too early.
DWDr. Worapakthorn Kongpesalaphun, M.D.Consultant Psychiatrist, One Step Rehab

Frequently Asked Questions About Inpatient vs Outpatient Rehab
Common questions about choosing between residential and outpatient addiction treatment.
Most inpatient programmes run 28–90 days. At One Step Rehab, the minimum recommended stay is 28 days. Shorter stays rarely work because detox alone takes 3–7 days, and the therapeutic work needed to build coping strategies and address underlying issues requires at least three weeks of structured engagement after stabilisation.
For severe addiction, yes. Research consistently shows higher completion rates and lower short-term relapse rates for residential treatment compared to outpatient, particularly for people with co-occurring mental health conditions, unstable home environments, or histories of multiple treatment attempts. For mild substance use issues with strong home support, outpatient can be equally effective.
Yes — that’s outpatient’s primary advantage. Sessions are scheduled around work, school, or caregiving. However, the flexibility can also be a limitation: daily life stress and trigger exposure continue during treatment, which is why outpatient works best either for milder addiction or as a step-down after completing residential treatment.
Mid-range residential rehab in Thailand costs approximately ฿280,000/month (~$8,500 USD) at One Step Rehab. This includes accommodation, all meals, therapy, fitness, medical oversight, and aftercare planning. Luxury facilities in Thailand charge $15,000–$30,000+/month. Budget options start around $2,000–$5,000/month but typically offer fewer therapy hours and less medical supervision.
After discharge, clients transition to aftercare — which may include outpatient therapy at home, regular check-ins with their One Step counsellor, alumni support groups, and a personalised relapse prevention plan. The transition from residential to independent living is the highest-risk period, which is why One Step’s aftercare programme maintains weekly contact for the first three months post-discharge.
Usually, yes. Most outpatient programmes require clients to be substance-free before therapy begins, which often means completing a separate medical detox. Inpatient programmes handle detox and therapy in one continuous process — you don’t need to arrange separate services. At One Step, detox is managed on-site with medical supervision before the full therapy programme begins.

Written by
Alastair Mordey
Alastair Mordey is one of the pioneers of drug and alcohol treatment globally and specifically in Asia. He has been an addiction’s professional for twenty years. He started his career as an expert in substance abuse w...
Learn more about Alastair
Medically reviewed by
Dr. Worapakthorn Kongpesalaphun
Consultant Psychiatrist · Thai Licensed Medical Doctor · Residency in Psychiatry, Somdet Chaopraya Institute · Doctor of Medicine, Rangsit University
Dr. Worapakthorn Kongpesalaphun is a Thai Licensed Medical Doctor and Expert in Preventive Medicine (Community Mental Health) with extensive experience in addiction treatment and public health management. He holds multip...
Learn more about Dr. Worapakthorn